Every November, Maria dreads the familiar descent. It starts subtly: the snooze button gets hit more often, the gym visits taper off, and carbohydrate cravings intensify. By December, she’s sleeping 10 hours a night but waking exhausted. Social invitations feel like burdens rather than opportunities. The joy she found in work, hobbies, and relationships dims like the winter light outside her window. She knows intellectually that spring will come, but emotionally it feels impossible.
Maria’s experience isn’t weakness or laziness. It’s Seasonal Affective Disorder (SAD), a recurrent pattern of major depression that emerges in fall or winter and remits in spring. Unlike general depression, SAD has a clear biological trigger: insufficient light exposure that disrupts circadian rhythms, neurotransmitter production, and hormonal balance. An estimated 10 million Americans experience SAD, with another 10-20% experiencing a milder form called the “winter blues.”
The standard treatment, a 10,000 lux light box used for 30 minutes each morning, helps many people. But research increasingly shows that SAD is a multi-system disorder requiring a multi-modal response. Light therapy addresses circadian misalignment, but what about the serotonin depletion, the social isolation, the thermal dysregulation, and the vitamin deficiencies that compound winter’s psychological burden? A comprehensive approach targets all these mechanisms, creating redundant support systems that make you resilient even when one intervention falls short.
Understanding the Circadian Drift
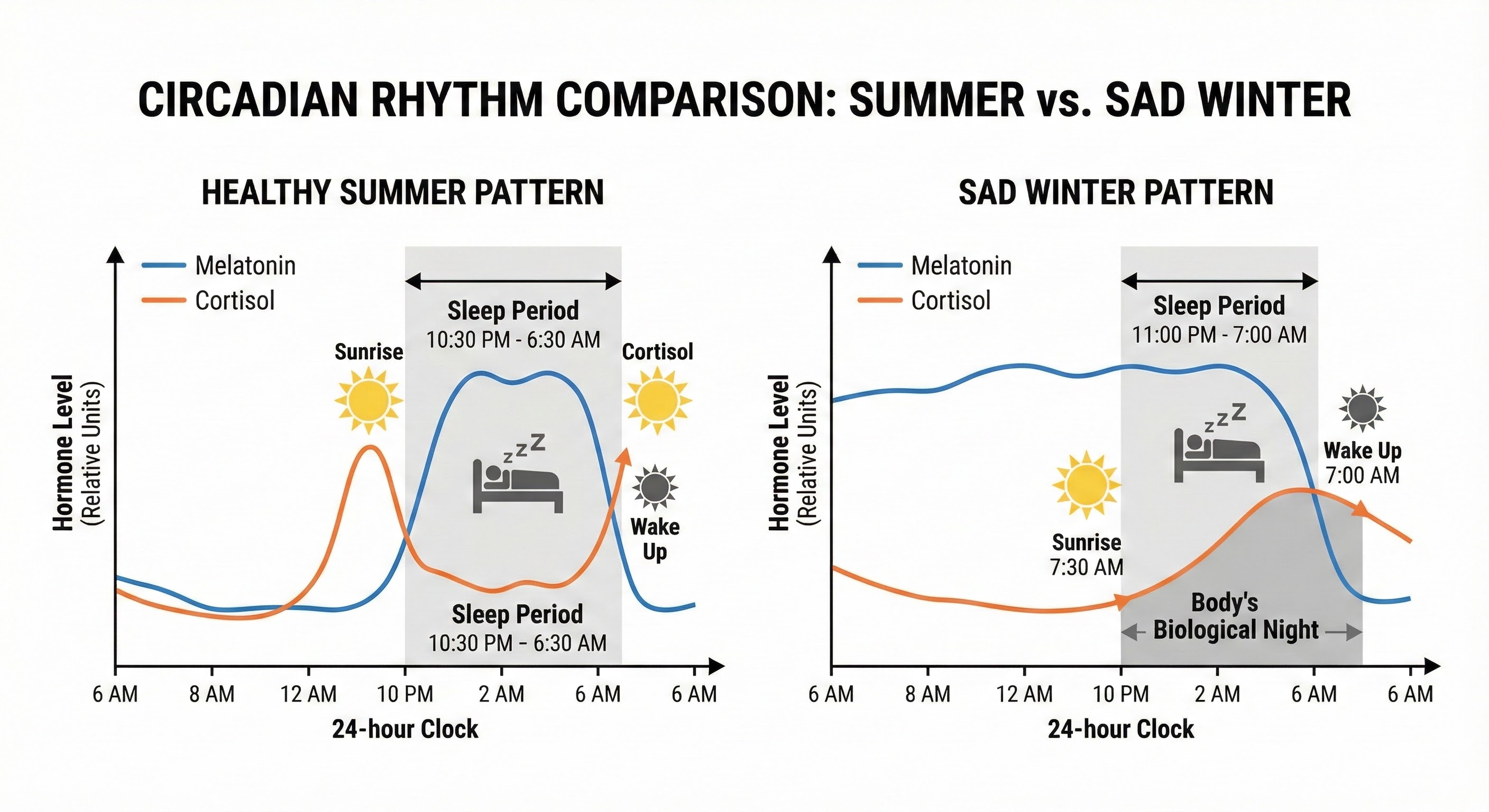
The core biological mechanism underlying SAD is circadian phase delay: your internal clock drifts later relative to the external day, creating a chronic state of jet lag. In summer, bright morning light signals your suprachiasmatic nucleus (SCN), the brain’s master clock, to suppress melatonin and initiate cortisol release, shifting you into alert daytime mode. In winter, the delayed and diminished sunrise leaves your SCN confused, continuing melatonin production well into the morning while you’re trying to function.
This phase delay explains the characteristic symptoms of SAD. The excessive sleep need reflects ongoing melatonin signaling that should have stopped hours earlier. The morning fatigue comes from blunted cortisol awakening response. The evening carbohydrate cravings represent your brain’s attempt to boost serotonin when light-dependent production pathways are compromised. Everything traces back to a clock that’s running late relative to social demands.
Light therapy works by providing the bright morning signal your SCN needs to reset. A 10,000 lux light box, used within an hour of waking for 20-30 minutes, can shift circadian phase earlier by several hours over 1-2 weeks. However, the effectiveness depends on precise timing and positioning. Many people use light therapy incorrectly, placing the box across the room or using it in the evening, actually worsening their phase delay rather than correcting it.
Understanding that SAD is fundamentally a circadian disorder also reveals why single interventions often disappoint. Your circadian system receives timing information from multiple sources: light exposure, meal timing, exercise, social interaction, and temperature fluctuations. A light box addresses one input while leaving others misaligned. The most effective SAD treatment protocols target multiple zeitgebers (time-givers) simultaneously, creating a coherent signal that your confused clock can interpret.
Optimizing Light Therapy: The Details That Matter
If you’re using a light box without results, the problem is likely technique rather than the modality itself. Research from the National Institute of Mental Health and multiple clinical trials has established specific parameters that distinguish effective light therapy from expensive window decoration.
Intensity and distance: The therapeutic dose is 10,000 lux at eye level, which requires the light source to be positioned 16-24 inches from your face. Light intensity drops exponentially with distance, so a light box across the room or in peripheral vision delivers perhaps 500 lux, far below therapeutic threshold. You don’t need to stare directly at the light, but it should be within your field of vision while you eat breakfast, read, or work on a computer.
Timing is critical: Light therapy must happen within the first hour after waking, ideally within 30 minutes. This timing anchors the phase-advance that corrects the circadian drift. Using light therapy after noon can actually shift your clock later, worsening symptoms and potentially causing insomnia as your brain interprets afternoon light as morning light from a delayed perspective.
Angle matters: The photoreceptors most connected to circadian regulation (melanopsin-containing intrinsically photosensitive retinal ganglion cells) are concentrated in the lower retina, which perceives light from above. Position your light box higher than your eyes, angled downward, to maximize circadian impact. Desktop positioning with the light at or below eye level is less effective than overhead placement.
Duration and consistency: Most research supports 20-30 minutes of daily exposure at 10,000 lux. Some people need longer (up to 60 minutes), while others respond to shorter sessions. Start with 30 minutes and adjust based on response over 2-3 weeks. Consistency matters more than perfection: daily use throughout the dark months produces better outcomes than sporadic marathon sessions.
Real outdoor light remains superior to any artificial source. Even on an overcast winter day, outdoor light intensity reaches 1,000-10,000 lux, compared to 100-500 lux in typical indoor environments. A 20-minute morning walk outside, even in cloudy conditions, provides light therapy alongside exercise, temperature exposure, and optic flow (the movement of visual scenery that independently regulates mood centers). This combination explains why outdoor exercise often outperforms isolated light therapy in SAD research.
The Thermal Connection: Why Cold Showers Help
People with SAD often report difficulty warming up in the morning, feeling perpetually chilled and sluggish. This isn’t imagined: research suggests that SAD involves impaired thermoregulation, with blunted morning body temperature rise contributing to the characteristic fatigue and lethargy.
Your circadian system and thermoregulatory system are intimately linked. Core body temperature normally rises in the morning (contributing to alertness) and falls in the evening (signaling sleep onset). In SAD, this rhythm flattens or delays, leaving you thermally stuck in “night mode” during the day. This provides another intervention target: deliberately manipulate body temperature to support circadian realignment.
A brief cold exposure upon waking, such as a 30-60 second cold shower or even splashing cold water on the face and hands, triggers a sharp sympathetic nervous system response. Noradrenaline and dopamine spike, body temperature rises during the subsequent rewarming, and alertness increases. Research on deliberate cold exposure demonstrates that the catecholamine release from cold water can elevate mood and energy for hours afterward, potentially compensating for the blunted neurotransmitter production characteristic of SAD.
Conversely, evening warmth can reinforce sleep timing. A warm bath 90 minutes before bed raises skin temperature, causing compensatory heat dissipation that drops core temperature over the following hour. This cooling signal promotes sleep onset and may improve the disrupted sleep architecture common in SAD. The contrast between morning cold and evening warmth creates a temperature rhythm that reinforces the light-based circadian signal.
This thermal approach isn’t about extreme discomfort. Brief cold exposure (even ending a warm shower with 30 seconds of cold water) and comfortable evening warmth (a bath, sauna, or heated blanket) represent accessible, low-cost interventions that address a mechanism light therapy doesn’t directly target. Combined with morning light, they create multiple synchronized signals pointing your confused circadian system toward proper alignment.

Nutritional Support for Winter Mood
SAD drives characteristic cravings for carbohydrate-rich comfort foods. This isn’t just emotional eating; it reflects your brain’s attempt to increase serotonin availability through dietary precursors. Tryptophan, the amino acid required for serotonin synthesis, crosses the blood-brain barrier more efficiently when insulin is elevated (which happens after carbohydrate consumption). The problem is that refined carbohydrates produce blood sugar spikes and crashes that ultimately worsen mood instability and fatigue.
Vitamin D supplementation is foundational for winter mood. Vitamin D receptors exist throughout the brain, including regions involved in mood regulation. A 2014 meta-analysis in the British Journal of Psychiatry found that vitamin D deficiency was associated with a 14% increased risk of depression and a 50% increased risk of suicide. Most people in northern latitudes become deficient during winter months when UVB radiation is insufficient for skin synthesis. Supplementation with 2,000-5,000 IU daily (adjusted based on blood testing) addresses this gap. For more on optimizing vitamin D levels specifically, see our guide on winter vitamin optimization.
Omega-3 fatty acids, particularly EPA (eicosapentaenoic acid), have demonstrated antidepressant effects in multiple trials. A 2019 meta-analysis in Translational Psychiatry found that omega-3 supplementation significantly reduced depressive symptoms, with higher EPA doses showing stronger effects. The mechanism involves anti-inflammatory effects (neuroinflammation is increasingly linked to depression) and potential modulation of neurotransmitter systems. A therapeutic dose is typically 1,000-2,000mg of EPA daily, either from fatty fish (salmon, mackerel, sardines) or high-quality fish oil supplements.
Rather than fighting carbohydrate cravings entirely, redirect them toward complex sources that provide the tryptophan-boosting effect without glycemic chaos. Root vegetables, steel-cut oats, quinoa, and legumes deliver sustained energy alongside the amino acid precursors your brain needs. Pair carbohydrates with protein at each meal to moderate insulin response while ensuring adequate tryptophan availability.
Strategic eating timing can reinforce circadian signals. Eating within an hour of waking (breakfast) and avoiding large meals close to bedtime creates a metabolic rhythm that supports the light and temperature signals you’re providing. Research suggests that late-night eating disrupts circadian alignment and may contribute to depressive symptoms independent of what you eat.
Social Rhythm Therapy: The External Clock
The tendency to hibernate during winter, to cancel plans and reduce social contact, exacerbates SAD through a mechanism called social rhythm disruption. Interpersonal and Social Rhythm Therapy (IPSRT), developed for bipolar disorder but applicable to SAD, recognizes that social interactions serve as powerful zeitgebers, external time cues that help stabilize circadian rhythms.
Every regular social commitment anchors your schedule to external time. Morning coffee with a partner, a weekly exercise class, a standing dinner date with friends, all create structure that prevents the drift into irregular sleep-wake patterns and social isolation that characterize SAD. When your internal clock is unreliable, external clocks provided by other people’s expectations become essential scaffolding.
IPSRT protocols involve tracking daily routines and social contacts, then deliberately stabilizing inconsistent elements. If you typically wake at different times on workdays and weekends (social jet lag), the intervention targets weekend wake times. If evenings have become isolated TV time, the protocol might add a twice-weekly dinner commitment. The goal isn’t rigid scheduling for its own sake but creating enough regularity that your circadian system receives consistent external input.
Research published in the American Journal of Psychiatry demonstrated that IPSRT reduced depression relapse rates in bipolar patients by stabilizing daily rhythms. While SAD is a different condition, the underlying circadian disruption responds to similar interventions. Social commitments that require you to wake at consistent times, leave the house, and interact with others create multiple circadian anchors beyond light exposure alone.
Practical implementation doesn’t require formal therapy. Schedule recurring commitments that require leaving home during morning hours: a gym class, a walking group, a breakfast meeting with a colleague. Protect these commitments as you would medical appointments. When the depressive pull toward cancellation hits, remember that the discomfort of socializing is temporary while the rhythm-stabilizing benefits accumulate over weeks.

Movement as Medicine: Exercise for SAD
Physical exercise is one of the most robust interventions for depression, including SAD. A 2016 meta-analysis in the Journal of Psychiatric Research found that exercise produced effects comparable to antidepant medications and psychotherapy, with benefits appearing within a few weeks of regular practice.
The mechanisms are multiple: exercise increases brain-derived neurotrophic factor (BDNF), which supports neuroplasticity and is depleted in depression; it elevates endorphins and endocannabinoids, producing immediate mood effects; it improves sleep quality, which is disrupted in SAD; and when performed outdoors, it combines with light exposure and social connection for compounded benefit.
Timing matters for SAD-specific benefits. Morning outdoor exercise provides light exposure, temperature manipulation (warming up from the cold), and circadian anchoring simultaneously. A 30-minute morning walk or jog, even on overcast days, may be more effective than an evening gym session of twice the duration because it addresses the specific circadian pathology underlying SAD.
Type of exercise matters less than consistency and enjoyment. Both aerobic exercise (walking, running, cycling) and resistance training have demonstrated antidepressant effects. Choose activities you’ll actually do when motivation is lowest. Group exercise classes provide social rhythm benefits alongside physical activity. Outdoor activities maximize light exposure benefit.
The motivation problem is the central challenge: SAD creates fatigue and anhedonia that make exercise feel impossible precisely when it’s most beneficial. Strategies include scheduling exercise appointments that others expect you to attend (accountability), starting with minimal commitments (a 10-minute walk rather than an hour at the gym), and using behavioral activation principles (acting despite not feeling motivated, rather than waiting for motivation to arrive).
When to Seek Professional Help
The interventions described in this article are supportive lifestyle practices, not replacements for professional treatment when SAD reaches clinical severity. If you’re experiencing thoughts of suicide or self-harm, profound inability to function at work or in relationships, or symptoms that don’t respond to lifestyle interventions within 4-6 weeks, consult a mental health professional.
Evidence-based professional treatments for SAD include:
Cognitive Behavioral Therapy for SAD (CBT-SAD) addresses the negative thought patterns and behavioral withdrawal that maintain depressive episodes. Research published in the American Journal of Psychiatry found that CBT-SAD was as effective as light therapy acutely and more effective at preventing relapse in subsequent winters. The skills learned in therapy, including behavioral activation and cognitive restructuring, transfer to future seasons.
Antidepressant medications, particularly SSRIs like bupropion (which has specific FDA approval for SAD prevention), can be helpful when lifestyle interventions are insufficient. Some people use prophylactic medication, starting in early fall before symptoms emerge and discontinuing in spring.
Light therapy under clinical supervision may be more effective than self-directed use, as clinicians can optimize timing, duration, and positioning based on individual response patterns. For severe SAD, combining light therapy with medication and/or psychotherapy produces better outcomes than any single intervention.
If you’ve experienced SAD in previous years, consider preventive action starting in early autumn before symptoms emerge. Beginning light therapy, vitamin D supplementation, and exercise commitments while you still have energy and motivation makes the interventions easier to maintain when darker days arrive.
The Bottom Line
Seasonal Affective Disorder is more than a bad mood that a lamp can fix. It’s a multi-system circadian disorder that responds best to multi-modal intervention. Light therapy addresses the core phase delay, but combining it with strategic temperature exposure, nutritional support, social rhythm stabilization, and regular exercise creates redundant support systems that make you resilient even when one intervention falls short.
Your winter resilience protocol:
- Morning light: Use a 10,000 lux light box within 30 minutes of waking, positioned 16-24 inches away and above eye level, for 20-30 minutes daily. Better yet, get outside for a morning walk when possible.
- Temperature contrast: Brief cold exposure upon waking (cold shower ending or face splash), warm bath or sauna in the evening 90 minutes before bed.
- Nutritional foundations: Vitamin D (2,000-5,000 IU daily based on blood levels), omega-3s (1,000-2,000mg EPA), complex carbohydrates over refined sources, and consistent meal timing.
- Social anchors: Schedule recurring morning commitments that require leaving the house and interacting with others. Protect these appointments as you would medical care.
- Move daily: Any exercise helps, but morning outdoor activity maximizes circadian benefit. Start with 10-minute walks if motivation is low.
- Seek help when needed: If symptoms persist despite lifestyle intervention, or if you’re experiencing thoughts of self-harm, consult a mental health professional immediately.
The goal isn’t perfect adherence to every recommendation but building enough supportive structure that the cumulative effect overcomes the biological pull toward darkness. Each intervention you implement adds another anchor holding your circadian system in place until the light returns.
Sources: Cell Reports Medicine on circadian mechanisms (2021), British Journal of Psychiatry meta-analysis on vitamin D and depression (2014), Translational Psychiatry meta-analysis on omega-3s and depression (2019), Journal of Psychiatric Research meta-analysis on exercise and depression (2016), American Journal of Psychiatry on CBT-SAD and IPSRT (multiple studies), National Institute of Mental Health light therapy guidelines, Dr. Norman Rosenthal (original SAD researcher) treatment protocols.