Depression costs the global economy over $1 trillion annually in lost productivity. Antidepressant medications help many people but leave roughly one-third of patients without adequate symptom relief, even after trying multiple drugs. Meanwhile, a dietary pattern originally developed in the 1920s to treat epilepsy has been accumulating evidence for psychiatric applications that the medical establishment is only now beginning to take seriously.
A systematic review and meta-analysis published in 2025 in JAMA Psychiatry, encompassing 50 studies and 41,718 participants, found that ketogenic diets were associated with significant reductions in depressive symptoms compared to control diets. Among the 10 randomized controlled trials specifically assessing depression, the effect was statistically significant and, in nonobese participants, the magnitude was large. A separate pilot study at a major university found a 69% reduction in standardized depression scores (PHQ-9) among college students following a ketogenic diet as adjunct therapy for major depressive disorder.
These findings arrive at a moment when nutritional psychiatry is moving from fringe concept to clinical discipline. The question is no longer whether food affects mood (it clearly does) but whether specific dietary patterns can serve as structured therapeutic interventions for psychiatric conditions. The ketogenic diet, with its unique metabolic properties, may be the strongest current candidate.
What Makes the Ketogenic Diet Different
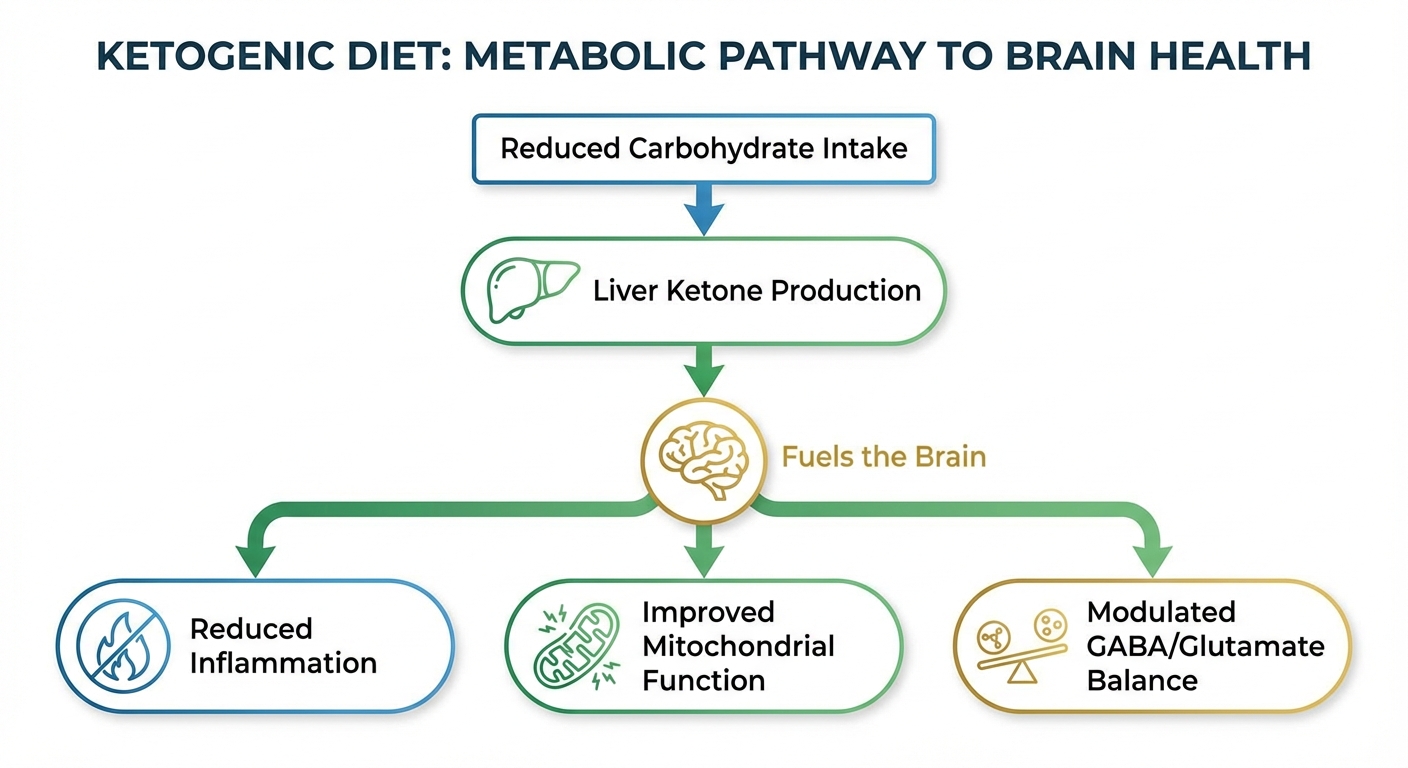
The ketogenic diet is not simply a low-carbohydrate diet. It is a metabolic intervention that fundamentally shifts the body’s primary fuel source from glucose to ketone bodies (beta-hydroxybutyrate, acetoacetate, and acetone), produced by the liver from fatty acids when carbohydrate intake drops below roughly 20-50 grams per day. This metabolic shift, called nutritional ketosis, produces biochemical changes throughout the body, with particularly pronounced effects in the brain.
The brain typically consumes about 120 grams of glucose daily, accounting for roughly 20% of the body’s total energy expenditure despite representing only 2% of body weight. During ketosis, ketone bodies provide up to 60-70% of the brain’s energy needs, with the remainder supplied by glucose produced through gluconeogenesis. This fuel switch is not a mere substitution: ketone bodies are metabolized differently than glucose, producing effects on mitochondrial function, oxidative stress, inflammation, and neurotransmitter balance that carry direct relevance to depression.
A standard ketogenic diet for therapeutic purposes typically contains approximately 70-80% of calories from fat, 15-20% from protein, and 5-10% from carbohydrates. The emphasis on fat comes from healthy sources: avocados, olive oil, fatty fish, nuts, and seeds. This is not a bacon-and-butter free-for-all. The quality of fats consumed matters for both physical health outcomes and, potentially, the neurological effects. A well-formulated therapeutic ketogenic diet looks nothing like the caricature version popular on social media.
The Meta-Analysis: What 50 Studies Reveal
The JAMA Network Open systematic review by Janssen Agular and colleagues searched MEDLINE, Embase, and APA PsycINFO through April 2025 and synthesized data from 50 studies totaling 41,718 participants. The inclusion of both observational and interventional studies provided a comprehensive picture of the association between ketogenic diets and mental health outcomes.
Among the 10 randomized controlled trials assessing depressive symptoms, ketogenic diets produced a statistically significant reduction compared to control diets. The effect was particularly strong in studies that verified biochemical ketosis (through blood or urine ketone measurement), indicating that the metabolic state itself, not merely carbohydrate restriction, drives the antidepressant effect. This distinction matters because it separates the ketogenic diet from generic “low-carb” approaches that may not achieve sufficient ketosis to trigger the relevant neurobiological changes.
A striking moderator finding: the association between ketogenic diets and depression improvement was larger and more significant in nonobese participants than in obese participants. This challenges the assumption that mood improvements from dietary changes are simply secondary to weight loss. Something about the ketogenic metabolic state itself appears to affect mood regulation independent of body composition changes.
The anxiety findings were more mixed. While some individual studies showed anxiety improvements, the meta-analytic result for anxiety symptoms did not reach statistical significance. The authors noted that anxiety and depression, while frequently comorbid, may respond differently to metabolic interventions, and that anxiety-specific trials with standardized outcome measures are needed.
Four Pathways: How Ketosis Affects Depression
The biological plausibility of the ketogenic diet’s antidepressant effects rests on multiple converging mechanisms, each supported by preclinical evidence and emerging human data.
Neuroinflammation reduction may be the most important pathway. Chronic low-grade brain inflammation has emerged as a leading mechanistic model for treatment-resistant depression. A 2024 review in Molecular Psychiatry documented elevated inflammatory markers (IL-6, TNF-alpha, CRP) in the cerebrospinal fluid of depressed patients, with the highest levels in those who did not respond to standard antidepressants. Beta-hydroxybutyrate (BHB), the primary ketone body, inhibits the NLRP3 inflammasome, a key driver of neuroinflammation. Dr. Shebani Sethi Dalai, a clinical associate professor at Stanford University Medical School who runs a metabolic psychiatry clinic, has described ketone bodies as “anti-inflammatory molecules that happen to also fuel the brain.” Her clinical research documents inflammation reduction as a consistent feature of patients who achieve sustained ketosis.
GABA/glutamate rebalancing provides another pathway. Depression and anxiety involve dysregulated balance between GABA (the primary inhibitory neurotransmitter, associated with calm and relaxation) and glutamate (the primary excitatory neurotransmitter, associated with activation and, in excess, neurotoxicity). Ketogenic diets increase GABA production and reduce glutamate levels through multiple mechanisms, including direct effects on the enzymes glutamic acid decarboxylase (GAD) and GABA-transaminase. This shift toward greater GABAergic tone is consistent with the anticonvulsant mechanism that originally justified the diet’s use in epilepsy, and it provides a plausible pathway for mood stabilization.
Mitochondrial function enhancement addresses the cellular energy deficit hypothesis of depression. Depressed patients consistently show reduced markers of mitochondrial function in brain imaging studies, suggesting that neurons in key mood-regulating regions are energy-deprived. Ketone bodies are a more efficient mitochondrial fuel than glucose: they produce more ATP per unit of oxygen consumed and generate fewer reactive oxygen species (free radicals) in the process. By improving cellular energy production in brain regions governing mood, motivation, and cognitive function, ketosis may address a root cause that conventional antidepressants do not directly target.
Gut-brain axis modulation adds a fourth pathway. The ketogenic diet substantially alters gut microbiome composition, and gut health is increasingly recognized as a driver of brain chemistry. A 2024 study in Nature Microbiology found that ketogenic diets reduced populations of pro-inflammatory gut bacteria while increasing Akkermansia muciniphila, a species associated with improved intestinal barrier function and reduced systemic inflammation. Changes in gut-produced neurotransmitters (serotonin, GABA, dopamine) following microbiome shifts could influence mood through the vagus nerve and immune signaling pathways.
The Stanford Metabolic Psychiatry Program
Dr. Shebani Sethi Dalai’s Metabolic Psychiatry Program at Stanford University School of Medicine represents the most prominent clinical effort to apply ketogenic dietary therapy to serious mental illness. Her program treats patients with schizophrenia, schizoaffective disorder, bipolar disorder, and treatment-resistant depression using medically supervised ketogenic diets.
In a Stanford Medicine report published in April 2025, Dr. Sethi Dalai shared five key insights from her clinical and research experience. The first is that the therapeutic mechanism appears to work through correcting metabolic dysfunction in brain cells. Using advanced brain imaging, her team has observed that patients with serious mental illness show patterns of impaired glucose metabolism in the brain that improve when ketone bodies become the alternative fuel source.
The second insight is that the diet works as adjunctive therapy, not as a replacement for psychiatric medication. Most patients in the Stanford program continue their prescribed medications while adding the ketogenic diet. The dietary intervention addresses metabolic dysfunction that medications do not target, creating a synergistic effect. Some patients eventually reduce medication doses under supervision, but this is a carefully managed process, not the goal.
Third, adherence is the primary challenge. Maintaining strict carbohydrate restriction is difficult, and the therapeutic effects appear to require sustained ketosis rather than intermittent compliance. Patients who achieve and maintain ketosis (verified by blood BHB levels above 0.5 mmol/L) show the most consistent improvements. The Stanford program provides dietitian support, meal planning assistance, and regular metabolic monitoring to address adherence challenges.
Practical Considerations: From Research to Application
The evidence, while growing, carries important caveats that should inform individual decision-making about dietary approaches to depression.
The meta-analysis authors explicitly state that “well-powered trials with standardized, verified protocols, structured support, and prespecified outcomes are needed to confirm efficacy and durability.” Current evidence is promising but not definitive. Most trials are small, short-term, and variable in their dietary protocols and adherence monitoring. The field needs large-scale, long-duration trials with standardized ketogenic protocols before dietary guidelines can formally recommend ketogenic diets for depression.
Medical supervision is essential for anyone considering a ketogenic diet for psychiatric purposes. The diet carries potential side effects including the “keto flu” (fatigue, headache, nausea during the adaptation period), kidney stone risk with long-term use, changes in lipid profiles (which can go in either direction depending on individual metabolism and food choices), and potential interactions with psychiatric medications. Antipsychotics and mood stabilizers that affect glucose metabolism may require dose adjustments when a patient enters ketosis.
The ketogenic diet is not appropriate for everyone with depression. Individuals with eating disorder histories, liver or kidney disease, or certain metabolic conditions should not pursue this approach without specialist guidance. The intensity of the dietary restriction can also exacerbate psychological rigidity or food anxiety in some individuals, potentially worsening the mental health condition it aims to treat.
For those interested in exploring the connection between diet and mood without the strict requirements of full ketosis, Mediterranean dietary patterns have their own evidence base for depression risk reduction, with a 2019 randomized trial (the SMILES trial, published in BMC Medicine) showing that a modified Mediterranean diet improved depression symptoms in one-third of participants to the point of remission.
A Lighter Touch: Nutritional Psychiatry Beyond Full Keto

Not everyone needs or can sustain full ketosis to benefit from the nutritional psychiatry insights embedded in this research. Several principles from the ketogenic diet evidence translate to less restrictive dietary adjustments that still support mental health.
Reduce refined carbohydrates and added sugars. The mechanism that makes ketogenic diets effective, stabilizing brain energy metabolism and reducing inflammation, operates on a spectrum. You do not need to eliminate carbohydrates entirely to reduce the blood sugar spikes and crashes that destabilize mood. Replacing refined grains and added sugars with whole food carbohydrates (vegetables, legumes, berries) reduces glycemic volatility and associated inflammation.
Prioritize omega-3 fatty acids. The brain is approximately 60% fat by dry weight, and omega-3 fatty acids (particularly DHA) comprise a significant portion of neuronal cell membranes. A 2019 meta-analysis published in Translational Psychiatry found that omega-3 supplementation (particularly EPA at doses of 1-2 grams daily) produced significant antidepressant effects, especially in patients already on antidepressant medication. Fatty fish, walnuts, flaxseed, and algae-derived supplements provide dietary omega-3s.
Support gut microbiome diversity. Fiber, fermented foods, and polyphenol-rich plants feed beneficial gut bacteria that produce neuroactive compounds. A 2024 randomized controlled trial published in Nature Communications found that six servings of fermented foods daily for 10 weeks significantly reduced inflammatory markers and improved self-reported mood in healthy adults.
Next Steps for Your Mind
The ketogenic diet’s effects on depression represent one of the most intriguing developments in nutritional psychiatry. The evidence has progressed from case reports and animal studies to a meta-analysis of 50 studies, and the biological mechanisms are plausible and converging. This is not “eat better, feel better” hand-waving. It is specific metabolic intervention with specific neurobiological effects.
If you are considering dietary approaches for depression:
- Talk to your psychiatrist or primary care physician before making changes, especially if you take psychiatric medications
- A medically supervised ketogenic trial, with blood ketone monitoring and dietitian support, provides the best information about whether the approach works for you individually
- If full keto is impractical, reducing refined carbohydrates, increasing omega-3 intake, and supporting gut health through fermented foods capture some of the relevant mechanisms
- Continue prescribed medications unless your provider recommends changes
What to expect realistically: Published studies show improvements emerging over 4-12 weeks of sustained ketosis. The adaptation period (first 1-2 weeks) is often uncomfortable. Consistent ketosis matters more than perfection; intermittent compliance may not produce the metabolic shifts associated with therapeutic benefit.
The convergence of metabolic science and psychiatric research is producing insights that neither field could generate alone. The ketogenic diet is not a cure for depression. But for the substantial population that does not respond adequately to conventional treatment, metabolic intervention through dietary change may represent a meaningful additional tool.
If you are experiencing depression, suicidal thoughts, or mental health crisis, please contact the 988 Suicide and Crisis Lifeline by calling or texting 988. The dietary information in this article is for educational purposes and does not replace professional mental health treatment.
Sources
- Janssen Aguilar, T. et al. “Ketogenic Diets and Depression and Anxiety: A Systematic Review and Meta-Analysis.” JAMA Psychiatry, 2025.
- Stanford Medicine. “Five key insights on keto therapy and mental illness.” Stanford Report, April 2025.
- Pilot study: “A pilot study examining a ketogenic diet as an adjunct therapy in college students with major depressive disorder.” PMC, 2025.
- American Journal of Managed Care. “Ketogenic Diets May Improve Depression Symptoms.” AJMC, 2025.