Picture a person in psychiatric crisis arriving at a typical emergency department. They’re placed in a curtained bay alongside patients with chest pain, broken bones, and abdominal emergencies. The lights are fluorescent and constant. Monitors beep. Staff rush past. The person may wait 8, 12, sometimes 24 hours or more for a psychiatric evaluation, often restrained or sedated, in an environment engineered to maximize medical throughput, not psychological stabilization. For someone experiencing a panic attack, psychotic episode, or suicidal ideation, the traditional ER is not just unhelpful. It actively makes things worse.
This is the environment that hospitals across the country are now working to fundamentally redesign. The movement isn’t happening because administrators suddenly developed empathy for psychiatric patients (though many have). It’s happening because the numbers leave no alternative. Mental health-related emergency department visits have surged over the past decade, psychiatric boarding (holding patients in the ER while waiting for inpatient beds that don’t exist) is consuming resources at unsustainable rates, and a growing body of evidence shows that specialized psychiatric emergency programs produce better outcomes at lower cost than the status quo.
The result is a quiet revolution in how American hospitals think about emergency psychiatric care: dedicated units with reclining chairs instead of gurneys, embedded psychiatric teams available around the clock, and crisis stabilization protocols that resolve 70 to 80% of cases within 24 hours without requiring inpatient admission.
The Scale of the Crisis
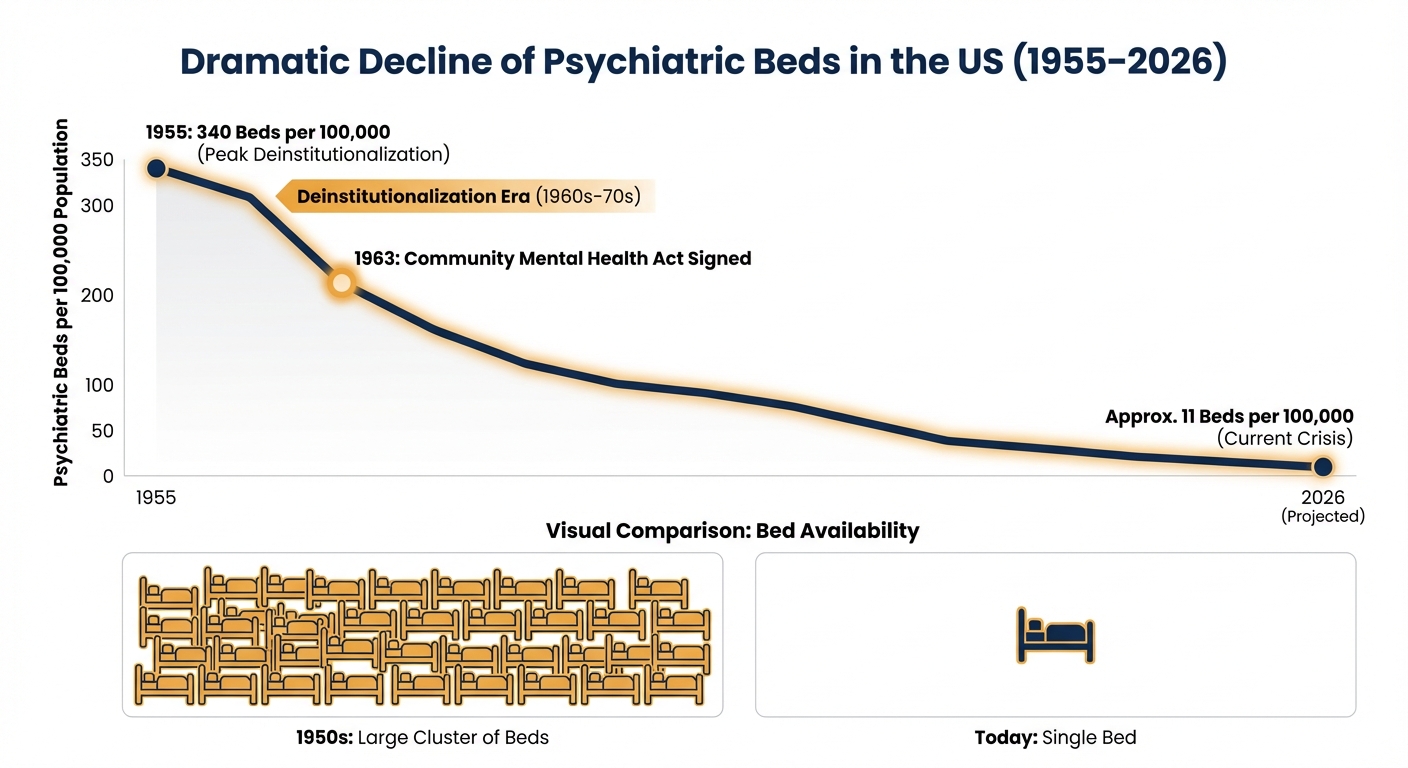
Emergency departments have become the de facto front door for mental health care in the United States, not because they’re designed for it, but because there’s nowhere else for many patients to go. The national shortage of psychiatric inpatient beds has been well-documented: the United States has approximately 11 psychiatric beds per 100,000 people, down from 340 per 100,000 in the 1950s. Community mental health centers are underfunded and overwhelmed. Outpatient wait times for psychiatrists routinely stretch to months. When someone is in acute crisis and can’t wait, the ER is the only option that’s open 24 hours and legally obligated to see them.
The consequences ripple through the entire emergency care system. Patients experiencing psychiatric emergencies who are “boarded” in the ER while waiting for an inpatient bed occupy rooms that could serve other patients. A 2024 analysis found that psychiatric boarding times averaged 10 to 24 hours in many hospitals, with some patients waiting days. During that time, they receive minimal psychiatric treatment because ER staff are trained in emergency medicine, not psychiatry. The patient deteriorates. The ER backs up. Everyone suffers.
Alicia Bunch, a behavioral health leader at University of Colorado Health, describes the shift hospitals are making: “Being able to identify risk and connect people to care has been really important.” The recognition driving reform is that the ER doesn’t need to become a psychiatric hospital. It needs to become a rapid assessment and stabilization point that routes patients to the right level of care within hours, not days. That requires fundamentally different spaces, staff, and protocols than what most emergency departments currently offer.
The EmPATH Model: Rethinking the Physical Space
The most visible change in psychiatric emergency care is architectural. EmPATH units, short for Emergency Psychiatric Assessment, Treatment and Healing, represent a new design philosophy that looks nothing like a traditional ER.
Dr. Scott Zeller, Vice President for Acute Psychiatry at Vituity and Assistant Clinical Professor of Psychiatry at the University of California, Riverside, has been one of the most vocal proponents of the model. EmPATH units blend “the wellness and recovery model with the medical model,” creating spaces that are simultaneously medically equipped and psychologically therapeutic. Instead of gurneys behind curtains, patients sit in recliners arranged in open living-room-style environments. Lighting is adjustable and warm rather than fluorescent. Sound levels are controlled. Staff are present and visible but not hovering. The environment is designed to de-escalate rather than contain.
The clinical rationale is straightforward. A person in psychiatric crisis needs safety, calm, and rapid assessment. The traditional ER provides none of these for psychiatric patients. Bright lights, loud noises, physical restraints, and long waits in isolation increase agitation, anxiety, and the likelihood of aggressive incidents. EmPATH units reverse these environmental triggers, and the outcomes data support the approach: programs report stabilization rates exceeding 75% for high-acuity psychiatric patients within 24 hours. Between 70% and 80% of patients are discharged directly to outpatient care or home without requiring inpatient admission.
That discharge rate is the key economic and clinical argument for EmPATH adoption. Every patient who stabilizes in an EmPATH unit and goes home with an outpatient follow-up plan is a patient who doesn’t occupy an inpatient psychiatric bed (which may not exist anyway) and doesn’t board in the ER for days waiting for one. The model is less expensive than inpatient admission, less resource-intensive than extended ER boarding, and produces better patient outcomes than either alternative.
Integrated Care Models That Work
Beyond the physical redesign, hospitals are implementing several integrated care models that embed psychiatric expertise directly into emergency department workflows.
Collaborative Care Models place multidisciplinary teams combining psychiatrists, primary care providers, and mental health specialists directly in the emergency department. A systematic review published in PMC analyzing 18 studies from 2013 to 2023 found that collaborative care models reduced psychiatric readmissions by 20% within 30 days of discharge and decreased inappropriate restraint use through improved crisis management. The trade-off is resource intensity: these models require substantial investment in staffing, training, and interdepartmental coordination.

Consultation-Liaison Teams take a slightly different approach, embedding psychiatric specialists who actively collaborate with ER physicians on cases involving mental health components. The same systematic review found that this model reduced physical restraint use by 15% compared to standard care and decreased overall ER wait times by approximately 20%. The limitation is scalability: trained psychiatric consultation-liaison professionals are in short supply, making this model difficult to implement in rural and resource-constrained settings.
Telepsychiatry addresses the scalability problem by bringing remote psychiatric consultations to emergency departments via videoconference. The evidence is encouraging: telepsychiatry reduces psychiatric consultation wait times by 30% and decreases ER overcrowding by 25%. For rural hospitals that may not have a single psychiatrist within 100 miles, telepsychiatry extends specialized care to patients who would otherwise receive none. The model depends on reliable internet infrastructure, which remains a barrier in some underserved areas, but adoption is accelerating rapidly.
Maria Jackson of Bournewood Health Systems captures the underlying philosophy: “Behavioral health is everywhere. EDs and ICUs have the highest incidents.” Mental health presentations don’t sort themselves neatly into separate facilities. They arrive at the same front door as every other emergency. The question is whether hospitals are prepared to treat them when they do.
Mobile Crisis Response: Keeping People Out of the ER
Some of the most promising developments are happening before patients ever reach the emergency department. Mobile crisis teams and co-response programs pair mental health professionals with law enforcement or EMS responders on calls involving psychiatric emergencies, with the goal of de-escalating situations in the community and connecting people to appropriate care without an ER visit.
New York City’s B-HEARD program (Behavioral Health Emergency Assistance Response Division) sends teams of medical and mental health professionals to nonviolent 911 mental health calls instead of police officers. The program, which NYC Health + Hospitals announced would be fully operated under the city’s hospital system beginning in spring 2026, represents a fundamental rethinking of who responds to mental health crises and where treatment begins.
The logic is compelling. Many people who present to emergency departments in psychiatric crisis don’t need emergency medical treatment. They need someone trained in crisis de-escalation, psychiatric assessment, and care navigation to help them access the right resource. When that person shows up at their door instead of a police officer, the trajectory of the crisis changes. Early data from mobile crisis programs across multiple cities show reductions in unnecessary ER transports, decreased law enforcement involvement in mental health calls, and improved patient satisfaction with the crisis response experience.
The challenge is scaling these programs to match demand. Mobile crisis teams require trained clinicians willing to work in the field during unpredictable hours, and the nationwide shortage of mental health professionals constrains every model of psychiatric care delivery, whether in the ER, the community, or telehealth platforms.
Prevention Over Crisis Response
The most forward-thinking health systems are moving beyond reactive crisis care toward identifying risk before patients reach the emergency department. Predictive modeling using electronic health record data can flag patients at elevated risk for psychiatric emergency based on patterns like missed appointments, medication refills that stop, or repeated ER visits for somatic complaints that may have underlying psychiatric drivers.
Routine mental health screening in primary care settings represents another prevention-oriented approach. When a family physician screens every patient for depression and anxiety at annual visits (using validated tools like the PHQ-9 and GAD-7), they can identify deteriorating mental health and intervene with outpatient treatment before a crisis occurs. This is dramatically less expensive and less traumatic than waiting for the patient to end up in the ER.
Ross Harper of Limbic, an AI-focused mental health technology company, argues that “clinically validated AI agents will be the great unlock” for behavioral health, enabling continuous monitoring and early intervention at a scale that human clinicians alone cannot achieve. Whether AI-driven mental health tools fulfill that promise or introduce new problems (data privacy, accuracy, over-reliance on technology) remains an open question. But the direction is clear: the goal is a system where emergency psychiatric care is the last resort, not the first contact.

Where to Start
The redesign of emergency psychiatric care is not a single policy change or hospital renovation. It’s a systemic shift happening across architectural design, staffing models, technology deployment, and community-based alternatives simultaneously. For individuals and families navigating mental health challenges, understanding what’s available can make a critical difference during a crisis.
If you or someone you know is in immediate psychiatric crisis:
- Call 988 (Suicide and Crisis Lifeline), which connects you to trained crisis counselors 24/7 by phone, text, or chat
- Ask your local ER whether they have a dedicated psychiatric emergency unit or EmPATH program, as these provide substantially better environments for psychiatric stabilization
- If available in your area, request a mobile crisis team response through 911 or your local crisis line instead of a standard ER visit
If you’re managing ongoing mental health conditions:
- Ask your primary care physician about routine depression and anxiety screening at your next visit
- Establish a relationship with an outpatient mental health provider before a crisis occurs, as having an existing treatment relationship improves crisis outcomes
- Discuss a crisis safety plan with your provider, including which emergency resources to use and in what order
- Consider telehealth psychiatry options if in-person access is limited in your area
For families and caregivers:
- Learn the signs of escalating psychiatric crisis (withdrawal, agitation, hopelessness expressed verbally, substance use increase)
- Familiarize yourself with your local hospital’s psychiatric emergency resources before you need them
- Save the 988 Suicide and Crisis Lifeline number in your phone now
The transformation of emergency departments from psychiatric holding areas into genuine treatment environments represents one of the most significant improvements in mental health care delivery in decades. It’s happening unevenly, with well-funded urban hospitals adopting new models faster than rural and under-resourced facilities. But the direction is consistent: better spaces, better-trained teams, faster stabilization, and a growing recognition that mental health emergencies deserve the same quality of care as physical ones.
If you’re experiencing persistent anxiety, depression, or other mental health concerns, consult a licensed mental health professional. The resources discussed here address crisis response and are not replacements for ongoing professional treatment.
Sources
- Psychiatric Times. “Hospital-Based Psychiatric Emergency Programs: The Missing Link for Mental Health Systems.” Dr. Scott Zeller.
- Becker’s Behavioral Health. “10 Trends Transforming Behavioral Health in 2026.”
- PMC. “Enhancing Emergency Room Mental Health Crisis Response: A Systematic Review of Integrated Models.” 2024.
- NYC Health + Hospitals. “Mayor Adams Announces New Model for B-HEARD Mental Health Crisis Response.” 2026.
- U.S. Senate. “Capito, Hassan Reintroduce Bill to Improve Mental Health Care in Emergency Departments.” 2026.