At 74, Margaret hadn’t done anything resembling exercise since her children were in elementary school. She accepted that weakness, fatigue, and difficulty rising from chairs were simply what happened when you got old. Her doctor had talked about something called sarcopenia, age-related muscle loss, but made it sound as inevitable as gray hair or wrinkles. Then her daughter enrolled her in a clinical trial, and two years later Margaret had gained four pounds of muscle, increased her strength by 35 percent, and stopped worrying about falling in her own home.
Sarcopenia affects 10 to 15 percent of adults over 60 and roughly half of those over 80. The consequences extend far beyond aesthetics. Low muscle mass predicts disability, falls, fractures, loss of independence, longer hospital stays, and earlier mortality. For decades, the medical establishment treated this progressive weakness as an unavoidable consequence of aging, something to be managed rather than reversed. New research proves this assumption wrong.
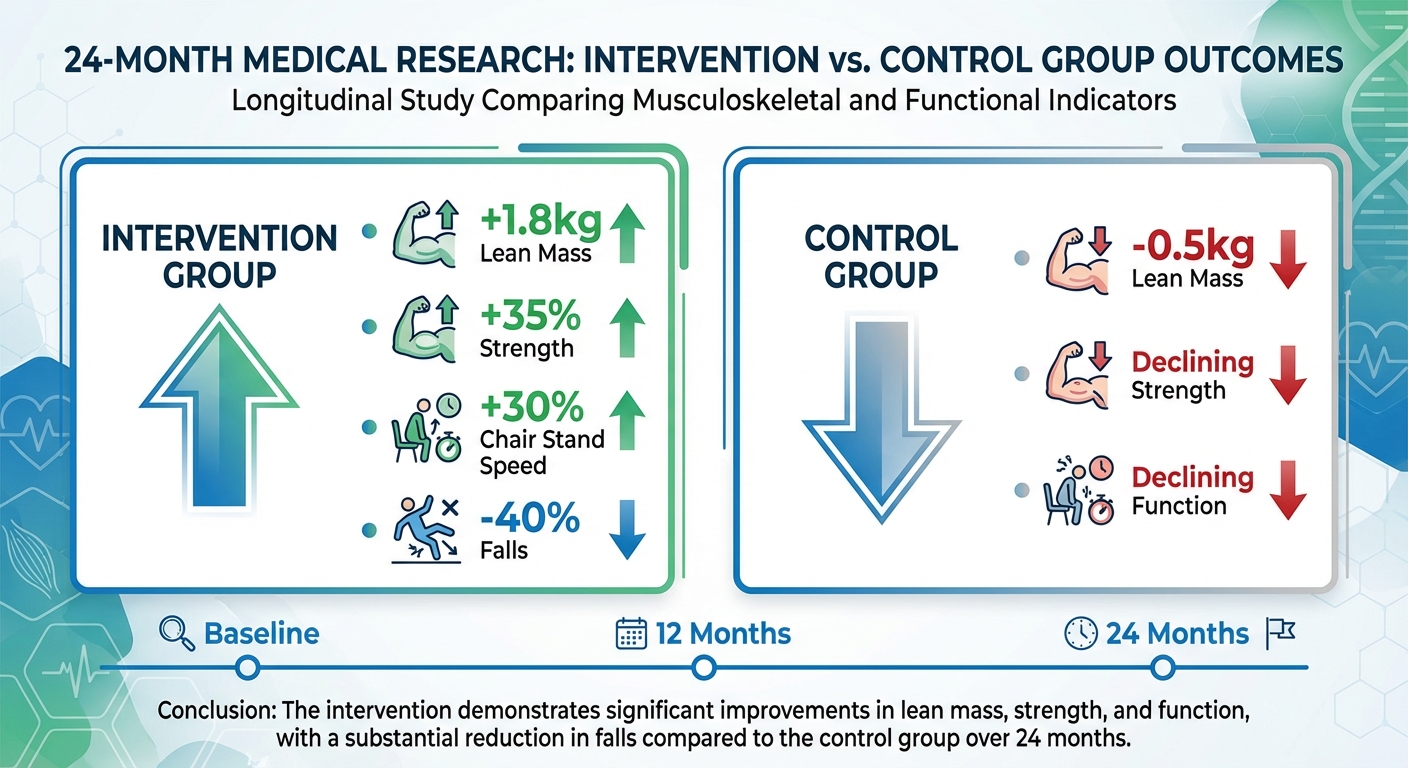
A landmark 2-year study of adults aged 70 to 85 demonstrated that high-protein intake combined with progressive resistance training doesn’t just slow muscle loss. It reverses it. Participants in the intervention group gained an average of 1.8 kilograms of lean mass, increased their strength by 25 to 40 percent across major movements, and saw dramatic improvements in functional capacity: easier standing from chairs, faster stair climbing, and 40 percent fewer falls. This happened in people who hadn’t exercised in decades, many of whom had multiple chronic conditions.
The message is both scientifically robust and personally empowering: sarcopenia is reversible at any age with proper intervention. Your seventies and eighties don’t have to be defined by progressive weakness.
The Landmark Study: Protocol and Results
To definitively answer whether severe muscle loss could be reversed in advanced age, researchers designed an intervention that challenged conventional wisdom about exercise for the elderly. Rather than prescribing gentle walking or light calisthenics, the protocol utilized rigorous resistance training adapted for safety but designed to drive real physiological adaptation.
The study enrolled 175 adults aged 70 to 85 who met clinical criteria for sarcopenia, meaning objectively low muscle mass and reduced strength or physical performance. Participants were randomly assigned to either an intervention group or a control group that received only general health advice. The intervention combined two elements: high protein intake at 1.6 grams per kilogram of body weight daily, roughly 110 to 130 grams for most participants, and progressive resistance training three times weekly focusing on major compound movements.
The resistance training wasn’t gentle. Participants performed leg presses, chest presses, rows, shoulder presses, and core exercises using weights that challenged them, starting conservatively but progressing systematically as they grew stronger. Sessions lasted 45 to 60 minutes. Trained instructors supervised initially, then participants continued independently with periodic check-ins to ensure proper form and appropriate progression.
After 24 months, the differences between groups were dramatic and clinically meaningful. The intervention group gained an average of 1.8 kilograms of lean mass while the control group lost an additional 0.5 kilograms, representing a net difference of over 2 kilograms of muscle tissue. Strength increased 25 to 40 percent across major lifts in the intervention group while declining slightly in controls. Time to rise from a chair improved 30 percent. Walking speed increased 15 percent. Falls decreased by 40 percent. Quality of life scores improved significantly across multiple domains.
The safety profile was remarkable given participants’ advanced age and deconditioned starting points. Adverse events were limited to minor muscle soreness, an expected and actually desirable sign of adaptation stimulus. No serious injuries occurred. No cardiovascular events were attributed to the exercise program. Even participants with multiple chronic conditions including diabetes, heart disease, and arthritis tolerated the program well with appropriate modifications.
The Physiology: Why This Combination Works
The intervention succeeded through the synergistic interaction of adequate protein and progressive mechanical loading, each addressing different components of the muscle-building equation that older adults struggle with.
Protein provides the essential building blocks, specifically amino acids, required for muscle protein synthesis. However, older adults develop what researchers call anabolic resistance: their muscles respond less robustly to protein intake than younger muscles do. Where a 25-year-old might maximally stimulate muscle protein synthesis with 20 to 25 grams of protein at a meal, a 70-year-old needs 30 to 40 grams to achieve the same anabolic response. The 1.6 grams per kilogram target ensures adequate amino acid availability throughout the day to overcome this blunted response and keep muscle protein synthesis elevated.
Resistance training provides the critical stimulus that signals the body to allocate those amino acids toward building new muscle tissue rather than simply burning them for energy. Without mechanical tension and the controlled damage that strength training creates in muscle fibers, extra protein doesn’t build muscle. The body has no reason to invest resources in tissue it doesn’t perceive as needed. Training creates the demand; protein supplies the materials to meet it.
Progressive overload, the systematic increase in weight or difficulty over time, prevents the adaptation plateau that would otherwise limit gains. Muscles adapt specifically to the loads placed on them. If someone starts lifting 30 pounds and continues lifting 30 pounds for two years, their muscles will adapt to that load within weeks and stop growing. By progressively increasing resistance as participants grew stronger, the protocol maintained continuous adaptation stimulus throughout the entire intervention period.
The time component matters particularly for older adults. Unlike young people who can build muscle relatively quickly when starting a training program, older adults’ gains accumulate more slowly. But two years of consistent work produces substantial total changes that transform functional capacity. The slow pace of adaptation in older muscle is exactly why shorter studies often underestimate what’s possible with sustained intervention.
For detailed guidance on protein timing to maximize muscle protein synthesis, our protein timing guide covers the research and practical applications.
Protein Requirements: Why Standard Recommendations Fall Short
For decades, dietary guidelines have recommended 0.8 grams of protein per kilogram of body weight for all adults, treating older adults as simply smaller versions of younger adults with proportionally scaled needs. This assumption has contributed to widespread sarcopenia by leaving older adults chronically under-proteinized during the life stage when protein needs are actually highest.

The discrepancy arises from efficiency differences. Young bodies are protein sponges, absorbing and utilizing amino acids with high efficiency after each meal. Older bodies are more like sieves, requiring larger protein boluses to trigger the same anabolic signaling cascades. An 80-year-old eating the same amount of protein as a 20-year-old will almost certainly lose muscle over time because the protein that maintains a young person’s muscle is insufficient to maintain an older person’s.
Emerging research supports substantially higher protein recommendations for older adults, in the range of 1.2 to 1.6 grams per kilogram, with the higher end appropriate for those actively trying to build muscle or recover from illness. For a 75-kilogram person, the sarcopenia-reversing target of 1.6 grams per kilogram translates to 120 grams of protein daily, roughly equivalent to four chicken breasts or 20 eggs, far more than most older adults currently consume.
Distribution across meals matters as much as total daily intake. Research suggests that spreading protein across three to four meals, with 30 to 40 grams at each feeding, maximally stimulates muscle protein synthesis throughout the day. Consuming most protein in a single large dinner meal, the typical pattern for many people, wastes the anabolic potential of the other meals and fails to keep muscle protein synthesis elevated during the hours between that dinner and the next day’s dinner.
For comprehensive information on protein needs across the lifespan, our protein requirements guide covers the evidence and practical implementation.
The Training Protocol: What Actually Works
The critical differentiator in successful sarcopenia intervention is the type of exercise prescribed. Staying active through gardening, walking, or gentle stretching provides genuine cardiovascular and mood benefits but creates insufficient mechanical tension to signal muscle growth. To reverse atrophy, muscle fibers must experience loads that challenge their current capacity.
Progressive resistance training forms the foundation of any evidence-based sarcopenia intervention. The study protocol had participants train three times weekly, typically on Monday, Wednesday, and Friday to allow adequate recovery between sessions. Each workout lasted 45 to 60 minutes and centered on compound movements that work multiple muscle groups simultaneously: leg press or squats for lower body pushing, rows for upper body pulling, chest press for upper body pushing, shoulder press for overhead strength, and core exercises for trunk stability.
The set and rep scheme followed standard hypertrophy protocols: 2 to 3 sets of 8 to 12 repetitions per exercise. Weight selection targeted a load that made completing 12 repetitions challenging but achievable with good form. When participants could complete 12 repetitions without significant difficulty, weight increased at the next session. This progressive overload principle is what drives continuous adaptation rather than quick plateau.
Supervision matters, particularly early in the process. Trained instructors taught proper form, ensured appropriate starting weights, and guided progression decisions. As participants developed competence and confidence, they transitioned to independent training with periodic check-ins to verify form hadn’t degraded and progression remained appropriate. This graduated autonomy model balances the safety benefits of supervision against the practical reality that most older adults won’t have access to indefinite personal training.
For readers interested in strength training fundamentals, our guide to strength training after 50 provides detailed programming recommendations.
Functional Benefits: Independence Preserved
While gaining 1.8 kilograms of lean mass represents a biological triumph, the true value of reversing sarcopenia is measured in independence and quality of life rather than muscle cross-sectional area. For older adults, muscle mass is the currency of autonomy. It determines whether you can rise from a toilet without assistance, carry your own groceries, and remain in your home rather than transitioning to assisted living.
The study documented striking functional improvements that translated directly to daily life. Chair stand time, a validated measure of lower body strength and power that predicts fall risk and functional status, improved by 30 percent in the intervention group. This isn’t an abstract metric. It’s the difference between struggling to stand from a low couch and rising smoothly without needing to push off the armrests. Walking speed increased 15 percent, improving the ability to cross streets before lights change and keep up with companions during social outings.
Most dramatically, fall incidence decreased by 40 percent in the intervention group compared to controls. Falls are the leading cause of injury death among adults over 65, and hip fractures from falls frequently initiate the cascade of decline that ends independence. Preventing falls isn’t just about avoiding injury in the moment; it’s about interrupting the pathway from fracture to hospitalization to rehabilitation facility to permanent loss of autonomy.
Participants reported feeling stronger, more capable, and more confident in their physical abilities. The psychological benefits of restored physical capacity compound the purely functional improvements. When you trust your body to support you, you move more, engage more socially, and maintain the activity levels that further reinforce physical capacity. Strength creates a positive feedback loop where capability generates more capability.
Barriers and Solutions for Implementation
If the solution to sarcopenia is relatively simple, lift weights and eat protein, why does the condition remain epidemic among older adults? The gap between scientific knowledge and real-world implementation is bridged by significant psychological, social, and structural barriers that must be addressed for widespread adoption.
Many older adults grew up in an era when strength training was associated with bodybuilders and athletes rather than general health. The concept of a 75-year-old grandmother lifting weights strikes some as strange or inappropriate, a cultural perception that has no basis in physiology but creates real hesitation. Education campaigns must normalize strength training for older adults as a health behavior equivalent to taking medication or getting regular checkups, not as something reserved for the athletically inclined.
Access barriers prevent many who would be willing to train from doing so. Gym environments can feel intimidating to deconditioned older adults unfamiliar with equipment. Transportation to fitness facilities may be challenging. Fixed incomes may not accommodate membership costs. Social isolation removes the encouragement and accountability that support adherence. These are addressable barriers through community-based programs, senior fitness classes designed for newcomers, home-based protocols, and family involvement in supporting older relatives’ exercise participation.

Home-based training offers a viable alternative for those without gym access or preference. Basic equipment costing $100 to $300, specifically resistance bands, adjustable dumbbells in the 10 to 30-pound range, and a sturdy chair, enables a complete sarcopenia intervention. Chair squats and sit-to-stands target the lower body muscles critical for functional independence. Dumbbell or band rows and presses work upper body pushing and pulling muscles. Wall push-ups progress to floor push-ups as strength improves. YouTube provides thousands of free instructional videos demonstrating proper form for older adult strength training.
Home training is admittedly less optimal than supervised gym-based training. Progression is harder to calibrate without equipment that increases in small increments. Motivation may flag without the social accountability of a gym environment. But home training is dramatically better than nothing, and for many older adults it represents the realistic path to participation that a gym-based recommendation never would.
Meeting the Protein Challenge
Prescribing 1.6 grams of protein per kilogram is simple on paper. Actually eating 120+ grams of protein daily is challenging for many older adults facing physiological and practical barriers to high protein consumption.
Appetite typically decreases with age due to changes in hunger hormones and taste sensation, a phenomenon called the anorexia of aging. Older adults often feel full more quickly and find large meals unappealing. Dental issues can make chewing fibrous meats difficult, steering people toward softer, often protein-poor alternatives. Reduced stomach acid production can make protein-rich meals feel heavy and difficult to digest. Social isolation leads many to adopt “tea and toast” eating patterns that provide calories but minimal protein.
Strategic food selection helps overcome these barriers. Greek yogurt provides 20 grams of protein per cup in a soft, easily consumed form. Cottage cheese offers 25 grams per cup. Eggs deliver 6 grams each and can be prepared in countless ways. Softer fish like salmon provides 25 grams per 4-ounce serving without requiring extensive chewing. For those who struggle to meet targets through food alone, whey or plant-based protein powder mixed into smoothies, oatmeal, or even soup adds 20 to 30 grams per serving without requiring a full meal.
Distribution strategy matters. Rather than trying to consume 120 grams in one or two meals, spreading intake across four eating occasions makes the target more achievable: 30 grams at breakfast (Greek yogurt with eggs or protein smoothie), 25 grams at lunch (chicken salad or cottage cheese with fruit), 35 grams at dinner (fish or meat with vegetables), and 20 grams as an evening snack (protein shake or cheese). This distribution also optimizes muscle protein synthesis by providing amino acids throughout the day rather than in a single bolus.
The Bottom Line
Sarcopenia is not an inevitable consequence of aging. It’s a condition that develops from inactivity and inadequate nutrition, and it reverses with the opposite: progressive resistance training and sufficient protein.
Adults in their seventies and eighties, including those who haven’t exercised in decades and those managing multiple chronic conditions, can build muscle, regain strength, and dramatically improve functional capacity with consistent intervention. The evidence is strong. The approach is safe when implemented appropriately. The benefits extend beyond muscle mass to fall prevention, maintained independence, and improved quality of life.
Your Sarcopenia Prevention Protocol:
-
Protein target: Consume 1.2 to 1.6 grams of protein per kilogram of body weight daily, distributed across 3-4 meals with 30-40 grams each.
-
Resistance training: Lift weights 2-3 times weekly focusing on compound movements: squats or leg press, rows, chest press, shoulder press.
-
Progressive overload: Increase weight when current loads become manageable. Continuous progression drives continuous adaptation.
-
Consistency over time: Gains in older adults are gradual but cumulative. Two years of consistent work produces transformative results.
-
Start regardless of age: Research shows benefits in adults through their eighties. The best time to start was years ago; the second best time is now.
If you’re over 60, this information applies directly to you. If you know someone over 65 who has accepted weakness as inevitable, share it with them. Sarcopenia reversal is possible, practical, and life-changing.
Sources: Clinical trials on sarcopenia reversal, protein requirements in older adults research, resistance training in elderly meta-analyses, functional outcomes and strength training studies, fall prevention research, International Society of Sports Nutrition position stands on protein for older adults.