The public conversation about GLP-1 receptor agonists has been dominated by before-and-after photos and celebrity weight loss stories since semaglutide first entered mainstream awareness in 2022. What gets far less attention is the question that matters more for long-term public health: what do these drugs do besides help people lose weight, and how strong is the evidence?
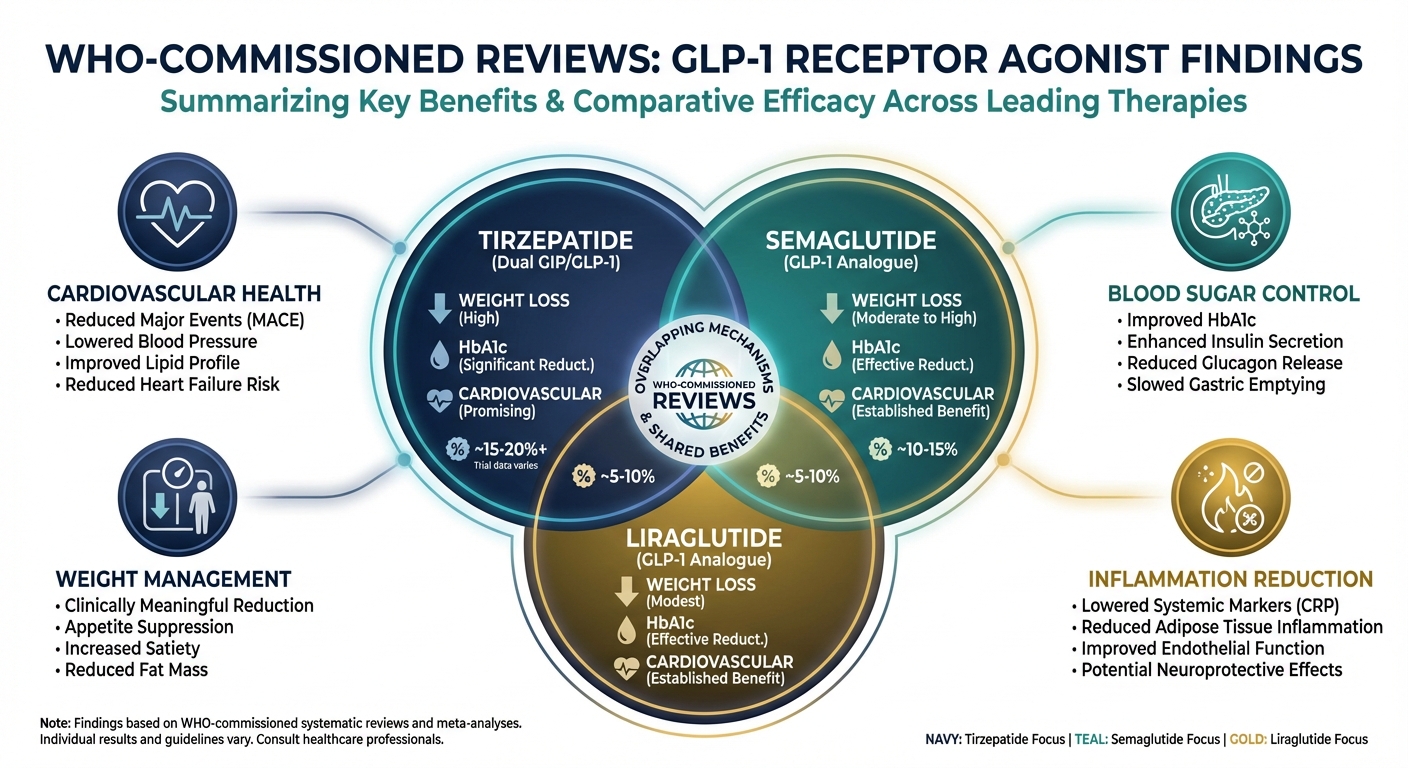
In early 2026, Cochrane, the global independent network known for rigorous systematic reviews, published three comprehensive analyses commissioned by the World Health Organization. The reviews were designed to inform WHO’s upcoming obesity treatment guidelines and together examined 50 randomized controlled trials enrolling more than 44,000 participants across three GLP-1 medications: tirzepatide, semaglutide, and liraglutide. The scope was deliberately broader than weight loss alone, evaluating cardiovascular outcomes, quality of life, adverse events, and mortality.
The results paint a more complex picture than either GLP-1 enthusiasts or skeptics typically present. These drugs produce substantial weight loss, particularly in the first year. But the cardiovascular benefits that have generated the most excitement are less clear-cut than headlines suggest, the long-term safety data remain limited, and the role of industry funding in shaping the evidence base deserves more scrutiny than it receives.
Three Drugs, Three Profiles
The WHO-commissioned reviews evaluated each GLP-1 medication separately, and the differences between them are clinically meaningful.
Tirzepatide (marketed as Mounjaro and Zepbound) produced the most dramatic weight loss. Across eight trials enrolling 6,361 participants, tirzepatide was associated with approximately 16% body weight reduction over 12 to 18 months. Tirzepatide is technically a dual GIP/GLP-1 receptor agonist, meaning it activates two incretin hormone pathways simultaneously, which likely explains its superior weight loss efficacy. Limited evidence suggests these effects may be sustained for up to 3.5 years, though the long-term data remain sparse.
Semaglutide (Ozempic for diabetes, Wegovy for weight management) showed roughly 11% weight loss over 24 to 68 weeks across 18 trials with 27,949 participants, the largest evidence base of the three drugs. The Cochrane reviewers found evidence suggesting effects can persist for at least two years, and semaglutide substantially increased participants’ likelihood of achieving the clinically meaningful 5% weight loss threshold.
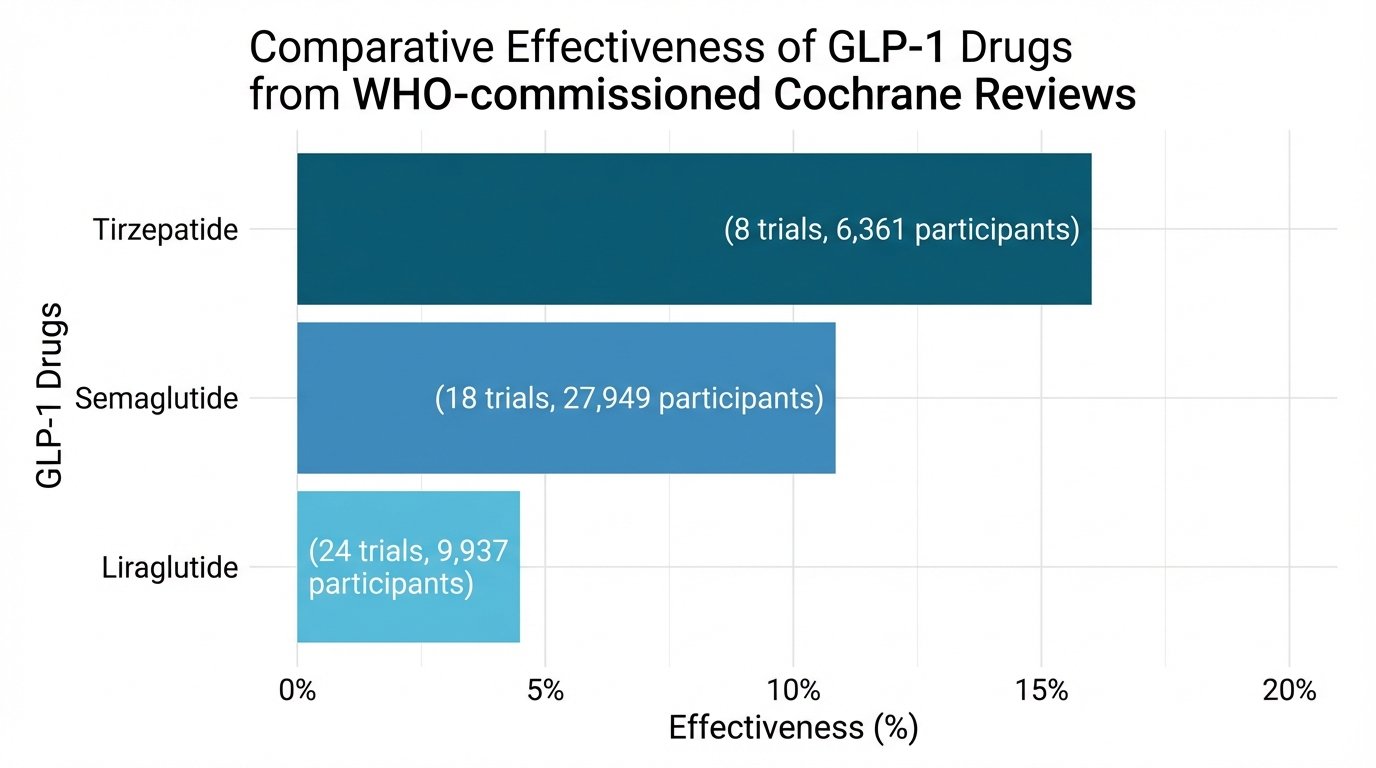
Liraglutide (Victoza for diabetes, Saxenda for weight management) delivered more modest results: 4 to 5% average weight reduction across 24 trials with 9,937 participants. While less dramatic than its newer counterparts, liraglutide still improved patients’ odds of achieving meaningful weight loss compared to placebo. Its significance in 2026 is partly economic: liraglutide’s patent has expired, allowing generic versions to enter the market at substantially lower prices. Semaglutide’s patent is also set to expire in 2026, which could reshape access dynamics for the most widely prescribed GLP-1 drug.
The Cardiovascular Question
The SELECT trial, published in 2023 in the New England Journal of Medicine, found that semaglutide reduced major adverse cardiovascular events (heart attack, stroke, or cardiovascular death) by 20% in adults with overweight or obesity and existing cardiovascular disease. This result generated enormous excitement and led to an expanded FDA indication for semaglutide covering cardiovascular risk reduction.
But the WHO-commissioned Cochrane reviews introduce important nuance. When the reviewers pooled all available evidence across the three drugs, they found “little to no difference” between GLP-1 medications and placebo when looking at major cardiovascular events, mortality, or quality of life in the broader study populations. The SELECT trial was specifically designed to test cardiovascular outcomes in a high-risk population with established cardiovascular disease. Most other GLP-1 trials were designed to measure weight loss, with cardiovascular events tracked as secondary outcomes in populations that may not have been at elevated cardiac risk.
Dr. Layla Abushamat of Baylor College of Medicine offers a mechanism-level perspective on why cardiovascular benefits might extend beyond weight loss. “Emerging research is examining heart-protective benefits of the drug itself, beyond weight loss,” she explains. GLP-1 receptor agonists improve blood sugar control, lower blood pressure, improve cholesterol profiles, and reduce inflammatory markers simultaneously. Adipose tissue functions as an endocrine organ, and excess fat drives chronic inflammation, insulin resistance, and dyslipidemia, all independent cardiovascular risk factors. By addressing multiple metabolic pathways at once, GLP-1 drugs may reduce cardiovascular risk through combined mechanisms rather than through weight loss alone.
The honest answer, as of early 2026, is that semaglutide has demonstrated cardiovascular benefit in one large, well-designed trial in patients with existing heart disease. Whether that benefit extends to the broader population of people taking GLP-1 drugs for weight management alone remains unproven. The evidence is promising but incomplete.
What the Reviews Don’t Tell Us
The Cochrane reviewers flagged several limitations that deserve more public attention than they typically receive.
Industry funding dominates the evidence base. The vast majority of included trials were funded by the drugs’ manufacturers, with substantial industry involvement in study planning, conduct, analysis, and reporting. Juan Franco of Heinrich Heine University, one of the review authors, acknowledged the potential and noted the call for independent studies: “Independent studies from a public health perspective are needed,” echoed Eva Madrid of Universidad de Valparaso, another review contributor. Industry funding doesn’t automatically invalidate results, but it introduces systematic biases in study design, outcome selection, and publication decisions that independent replication would help address.
Long-term data are limited. Most trials lasted 12 to 18 months. The longest follow-up for tirzepatide extends to roughly 3.5 years, but with limited participant numbers at that duration. For drugs that patients may take for decades, the absence of five-year and ten-year safety data represents a significant gap. Weight regain after discontinuation is well-documented, with research suggesting approximately two-thirds of lost weight returns after stopping GLP-1 therapy, raising the question of whether these are lifelong medications for most users.
Geographic representation is narrow. Research has been concentrated in middle- and high-income countries, with minimal representation from Africa, Central America, and Southeast Asia. Obesity is a global condition, and treatment guidelines informed primarily by data from North American and European populations may not generalize to all contexts. Genetic variation in GLP-1 receptor expression, dietary patterns, and comorbidity profiles could all influence how these drugs perform in underrepresented populations.
Side effects are common. Gastrointestinal adverse events, primarily nausea, vomiting, and diarrhea, were consistently more frequent in drug groups than placebo groups across all three reviews. Some participants discontinued treatment due to these effects. Additional safety considerations include potential muscle loss (particularly concerning for older adults), increased heart rate, and contraindications for people with personal or family history of medullary thyroid cancer.
The Expanding GLP-1 Landscape
While the WHO-commissioned reviews focused on weight and cardiovascular outcomes, a parallel body of research is exploring GLP-1 drugs for conditions that have nothing to do with obesity.
The SELECT trial’s cardiovascular findings have already expanded semaglutide’s FDA-approved uses. But researchers are also investigating GLP-1 receptor agonists for metabolic dysfunction-associated steatotic liver disease (MASLD, formerly NAFLD), kidney disease progression, neurodegenerative conditions including Alzheimer’s disease, and even addiction. GLP-1 receptors are expressed throughout the body, not just in the pancreas and gut, which provides biological plausibility for effects across multiple organ systems.
The kidney data are among the most intriguing. The FLOW trial, focused on semaglutide in patients with type 2 diabetes and chronic kidney disease, was stopped early due to efficacy, meaning the drug was working well enough that continuing to give some patients placebo was considered unethical. If confirmed in broader populations, kidney protection could become one of the most significant GLP-1 applications beyond weight management.
For people tracking their metabolic health through emerging technologies, these expanded indications matter because they reframe GLP-1 drugs from weight loss tools to potential multi-system metabolic therapies. That reframing also carries risk: the broader the claimed benefits, the stronger the incentive for off-label prescribing in populations where the evidence doesn’t yet support use.
What This Means for You
The access question is evolving rapidly. High prices have restricted tirzepatide and semaglutide to patients with insurance coverage or substantial out-of-pocket budgets. Monthly costs without insurance can exceed $1,000. But liraglutide’s patent expiration has already brought generics to market at lower price points, and semaglutide’s 2026 patent expiration could similarly expand access. Whether generic semaglutide becomes widely available in 2026 or 2027 depends on regulatory and legal factors still in play.
For patients currently using or considering GLP-1 medications alongside lifestyle interventions, the WHO-commissioned reviews suggest several evidence-based takeaways. These drugs work for weight loss, with tirzepatide producing the largest effect and liraglutide the most modest. Cardiovascular benefits are established for semaglutide in patients with existing heart disease but not conclusively demonstrated in the general population. Side effects are common enough that they should be discussed with your prescribing physician before starting. And the long-term picture, including what happens to your weight, cardiovascular markers, and overall health after years of use or upon discontinuation, remains genuinely uncertain.
What the Research Tells Us
The WHO-commissioned Cochrane reviews represent the most comprehensive independent analysis of GLP-1 drugs to date, and their conclusions are appropriately measured. These medications produce meaningful weight loss. They appear safe over 12 to 18 months. They may offer cardiovascular and metabolic benefits beyond weight reduction. But the evidence for long-term safety is incomplete, most of the existing data come from industry-funded trials, and the populations studied don’t yet reflect the full diversity of potential users.
The practical implications come down to three points:
- GLP-1 drugs are effective weight loss medications, not miracle drugs. Tirzepatide at 16% body weight reduction and semaglutide at 11% are clinically significant outcomes. They are not cures for obesity, and weight regain upon discontinuation is common.
- Cardiovascular benefits are real but context-dependent. If you have existing cardiovascular disease, the evidence for semaglutide’s cardioprotective effects is strong. If you’re otherwise healthy and considering GLP-1 drugs primarily for weight loss, the cardiovascular benefit is less certain.
- Independent research is urgently needed. The call from Cochrane reviewers for publicly funded, independent trials is not a formality. It’s a recognition that the evidence base for drugs used by millions of people should not be primarily generated and controlled by the companies selling them.
For patients navigating these decisions, the honest summary is this: GLP-1 drugs are the most effective pharmacological weight loss tools we have. The emerging evidence for benefits beyond weight is intriguing but not yet definitive. Long-term safety data will take years to accumulate. And the decision to start, continue, or stop these medications should be made with a physician who understands both the evidence and your individual health profile.
This article discusses current research findings and is not medical advice. Consult your healthcare provider before starting, stopping, or modifying any medication.
Sources
- Cochrane. “GLP-1 Drugs Effective for Weight Loss, But More Independent Studies Needed.” 2026.
- MedicalXpress. “GLP-1 Drugs May Protect the Heart Beyond Weight Loss, Trial Results Suggest.” February 2026.
- ScienceDaily. “Blockbuster Weight Loss Drugs Like Ozempic Deliver Big Results but Face Big Questions.” February 2026.
- NPR. “What’s Ahead for the Weight-Loss Drugs Known as GLP-1s in 2026.” January 2026.
- Cleveland Clinic. “GLP-1 Agonists: What They Are, How They Work & Side Effects.”