For the 3.1 million Americans living with inflammatory bowel disease (IBD), the relationship between eating and pain is intensely personal. Every meal carries a calculation: will this trigger a flare? Will this calm things down? For decades, dietary interventions for Crohn’s disease have been frustratingly vague, usually amounting to “avoid foods that bother you.” Two clinical trials published in early 2026 offer something far more specific, and the results are striking enough to shift how gastroenterologists think about diet as a therapeutic tool.
A randomized controlled trial led by researchers at the University of Calgary, published in February 2026, found that time-restricted eating (an eight-hour eating window) reduced Crohn’s disease activity by 40% and cut abdominal discomfort in half over 12 weeks. Separately, a randomized controlled trial published in Nature Medicine in January 2026 found that a fasting-mimicking diet (severely restricted calories for five days per month) achieved clinical response in 69% of Crohn’s patients and remission in over 60%. Both trials used rigorous methodology, active control groups, and validated outcome measures.
These are not marginal effects. A 40% reduction in disease activity and a 69% clinical response rate compete favorably with some pharmaceutical interventions for mild-to-moderate Crohn’s disease, though with important caveats about patient selection, study size, and the need for replication.
The Time-Restricted Eating Trial
The University of Calgary study, conducted at multiple Canadian sites and reported by the Crohn’s & Colitis Foundation, enrolled 35 adults with active Crohn’s disease who were also overweight or obese. Twenty participants were randomized to time-restricted feeding (TRF), limiting all food intake to an eight-hour daily window, while 15 continued their normal eating patterns. The trial ran for 12 weeks with standardized outcome assessments.
The primary finding was a 40% reduction in Crohn’s Disease Activity Index (CDAI) scores in the TRF group, compared to no significant change in controls. CDAI is the standard clinical tool for measuring Crohn’s disease severity, incorporating symptoms like abdominal pain, diarrhea frequency, general well-being, and complications. A 40% reduction moves many patients from moderate disease activity into mild or remission categories.
Abdominal discomfort, a symptom that directly affects quality of life, decreased by 50% in the fasting group. This is a clinically meaningful reduction for patients who structure their daily lives around managing pain. The TRF group also showed improved blood markers of inflammation, including lower levels of leptin (an inflammatory adipokine) and plasminogen activator inhibitor-1 (PAI-1, linked to both inflammation and clotting risk).
Body weight changed in both groups but in opposite directions: TRF participants lost an average of 5.5 pounds, while controls gained approximately 3.7 pounds. This divergence matters because excess adipose tissue is itself pro-inflammatory, producing cytokines that can drive Crohn’s flares. The weight loss in the TRF group may partially explain the anti-inflammatory effects, though the inflammatory marker improvements exceeded what weight loss alone would predict.
The study’s limitations deserve honest acknowledgment. The sample size of 35 is small by clinical trial standards. The study was not blinded (participants knew whether they were fasting), introducing potential placebo and behavior modification effects. The population was specifically overweight or obese, so results may not generalize to normal-weight Crohn’s patients. And 12 weeks, while sufficient to detect short-term changes, does not tell us whether the benefits persist over years.
The Fasting-Mimicking Diet Trial
The second trial, published in Nature Medicine by Dr. Valter Longo’s group at the University of Southern California in collaboration with Stanford Medicine, tested a different fasting approach: the fasting-mimicking diet (FMD). Rather than daily time restriction, FMD involves eating a severely calorie-restricted, plant-based diet (700 to 1,100 calories per day) for five consecutive days each month, then eating normally for the remaining 25 days.
This randomized controlled trial enrolled 97 participants with mild-to-moderate Crohn’s disease. Half followed the FMD protocol; half ate their normal diet. The results were noteworthy: 69% of patients on the fasting-mimicking diet achieved clinical response (a meaningful reduction in symptom scores), and over 60% reached clinical remission. In the control group, 44% showed clinical response, a difference that reached statistical significance.
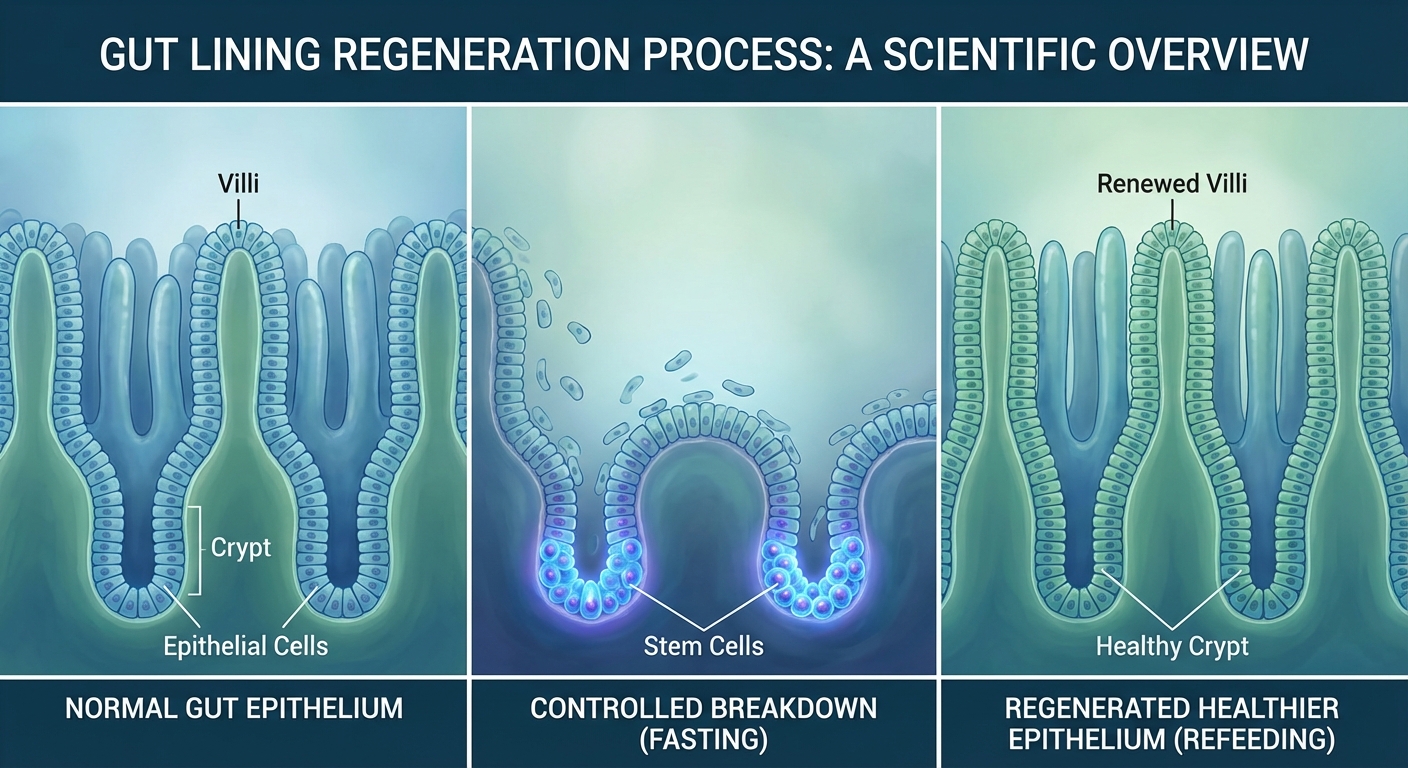
The mechanism proposed by Longo and colleagues centers on intestinal stem cell regeneration. Previous research in animal models demonstrated that fasting cycles trigger a process where the gut lining partially degrades during the fasting period, then regenerates from stem cells during refeeding. This cycle of controlled damage and repair appears to “reset” the intestinal lining, producing a less inflammatory mucosal environment. The clinical trial confirmed that fasting-mimicking diet participants showed reduced markers of intestinal inflammation alongside their symptom improvements.
A critical detail: the fasting-mimicking diet was specifically designed to provide enough nutrition to be safe while still triggering the fasting-associated metabolic switch from glucose metabolism to fatty acid oxidation and ketogenesis. The diet is high in plant fats, low in protein and carbohydrates, and supplemented with specific micronutrients. This is not simply “eating less.” The macronutrient composition matters for triggering the biological pathways associated with fasting’s therapeutic effects.
How Fasting Reduces Intestinal Inflammation
Understanding the mechanisms behind these results helps evaluate their significance and applicability. Fasting affects the gut through at least four distinct pathways, each supported by preclinical and emerging clinical evidence.
Autophagy activation is the most studied mechanism. During extended fasting (typically beyond 14-16 hours), cells activate autophagy, a cellular recycling process that degrades damaged proteins, dysfunctional organelles, and intracellular debris. In the gut lining, autophagy helps clear damaged cells and inflammatory mediators. Impaired autophagy has been directly linked to Crohn’s disease pathogenesis: the ATG16L1 gene, one of the strongest genetic risk factors for Crohn’s, encodes a protein essential for autophagy. Fasting, by upregulating autophagy, may compensate for genetic autophagy deficits in susceptible individuals.
Microbiome modulation occurs during fasting periods. Time-restricted eating shifts the composition of gut bacteria, generally increasing populations associated with anti-inflammatory short-chain fatty acid production (particularly Akkermansia muciniphila and Faecalibacterium prausnitzii) and decreasing populations associated with pro-inflammatory metabolites. A 2025 study in Gut Microbes demonstrated that even four weeks of 16:8 time-restricted eating produced measurable microbiome shifts in healthy adults, with changes correlating to improved intestinal barrier function markers.
Intestinal barrier repair connects the microbiome changes to clinical improvement. The “leaky gut” phenomenon, where tight junctions between intestinal epithelial cells loosen and allow bacterial products to cross into the bloodstream, is a hallmark of Crohn’s disease. Fasting-associated microbiome changes support tight junction integrity, while autophagy clears damaged epithelial cells. The combination improves barrier function, reducing the translocation of bacterial endotoxins that trigger systemic inflammation.
Immune cell reprogramming represents the most intriguing mechanism. Research from Longo’s lab, published in Cell Stem Cell, showed that fasting cycles reduce circulating white blood cell counts during the fasting period, then trigger stem cell-based immune regeneration during refeeding. The newly generated immune cells show a less inflammatory phenotype than those they replaced. In Crohn’s disease, where the immune system mistakenly attacks intestinal tissue, this immune “reset” could redirect immune activity away from self-destructive patterns.
Who Might Benefit and Who Should Be Cautious
These results do not mean every Crohn’s patient should start fasting tomorrow. Patient selection, medical supervision, and individual disease characteristics all matter for determining who is likely to benefit and who faces unacceptable risk.
The strongest evidence applies to patients with mild-to-moderate Crohn’s disease. Both trials excluded patients with severe or complicated disease (strictures, fistulas, recent surgery). Patients with active severe inflammation, malnutrition, or underweight should not fast without direct medical supervision, as caloric restriction carries real risk of worsening nutritional deficits that already accompany active Crohn’s disease.
The Calgary trial specifically enrolled overweight and obese patients, for whom the metabolic effects of fasting (weight loss, reduced adipose tissue inflammation) provide additional benefits beyond the gut-specific mechanisms. Normal-weight or underweight patients may not experience the same degree of improvement, and the risk-benefit calculation shifts accordingly.
Drug interactions require consideration. Many Crohn’s patients take immunomodulators, biologics, or corticosteroids, and fasting could alter drug metabolism, absorption timing, or immune function in ways that interact with these medications. Any fasting protocol should be coordinated with the prescribing gastroenterologist.
Populations who should proceed cautiously or avoid fasting:
- Patients with severe or complicated Crohn’s disease
- Underweight or malnourished individuals
- Patients with a history of eating disorders
- Pregnant or breastfeeding women
- Children and adolescents (insufficient safety data)
- Patients on medications requiring food for proper absorption
The broader context matters too. Intermittent fasting has accumulated substantial evidence for metabolic health benefits in general populations, but applying fasting to a specific disease population requires disease-specific evidence, which these trials are beginning to provide.
What This Changes for Crohn’s Management
These trials represent a shift from anecdotal dietary advice to evidence-based dietary intervention for inflammatory bowel disease. Several implications emerge for clinical practice and ongoing research.
First, the evidence supports incorporating structured fasting discussions into gastroenterology care for appropriate patients. This does not mean replacing pharmaceutical therapies, which remain the standard of care for moderate-to-severe Crohn’s disease. It means adding a dietary intervention with growing clinical evidence as a complementary approach, particularly for patients with mild disease who want to minimize medication use or for patients on stable regimens seeking additional symptom improvement.
Second, larger confirmatory trials are needed. Both studies are promising but preliminary. The Calgary trial enrolled 35 patients; the Nature Medicine trial enrolled 97. Gastroenterology guidelines require larger, multicenter trials with longer follow-up before dietary interventions receive formal clinical recommendations. Several such trials are now in planning or recruitment phases, including a UBC Okanagan study examining time-restricted eating in Crohn’s patients with overweight that reported initial results in February 2026.
Third, the mechanism research opens new therapeutic targets. If autophagy activation, microbiome modulation, and immune reprogramming are confirmed as key pathways, it becomes possible to develop pharmacological agents that mimic fasting’s benefits without requiring caloric restriction. Longo’s fasting-mimicking diet represents an intermediate step: providing the metabolic triggers of fasting while allowing some food intake, making compliance more sustainable than total caloric restriction.
The Evidence, Summarized
Two randomized controlled trials published in early 2026 provide the strongest clinical evidence to date that structured fasting can meaningfully reduce Crohn’s disease symptoms and intestinal inflammation. The 40% disease activity reduction with time-restricted eating and the 69% clinical response rate with fasting-mimicking diet represent clinically significant effects backed by plausible biological mechanisms.
Key takeaways for patients with Crohn’s disease:
- Discuss fasting-based approaches with your gastroenterologist before starting any protocol
- Time-restricted eating (16:8 protocol) and fasting-mimicking diets (five days per month) have the strongest current evidence
- These approaches appear most applicable to mild-to-moderate disease in patients who are overweight
- Fasting does not replace prescribed medications but may serve as a complementary strategy
- Monitor symptoms closely and discontinue fasting if symptoms worsen
For the broader research community, these trials validate dietary intervention as a legitimate therapeutic strategy for IBD and justify the larger-scale trials needed to establish clinical guidelines. The intersection of gut health science, metabolic research, and immunology is producing insights that could transform management of a disease that affects millions.
Always consult your healthcare provider before making dietary changes if you have inflammatory bowel disease or any chronic health condition. The information presented here summarizes published research and does not constitute medical advice.
Sources
- Wei, S. et al. “A fasting-mimicking diet in patients with mild-to-moderate Crohn’s disease: a randomized controlled trial.” Nature Medicine, January 2026.
- University of Calgary / Crohn’s & Colitis Foundation. “Intermittent Fasting Cut Crohn’s Disease Activity by 40% and Halved Inflammation in Randomized Clinical Trial.” February 2026.
- Stanford Medicine / Department of Medicine. “A Five-Day-a-Month Diet Shows Promise for Crohn’s Disease Relief.” 2026.
- University of British Columbia Okanagan. “Time-restricted eating shows promise for overweight people living with Crohn’s.” February 2026.