The COVID-19 pandemic became an unintended global experiment in nutritional epidemiology. As hospitals filled and researchers scrambled to identify risk factors, one pattern emerged with striking consistency across continents and demographics: patients with vitamin D deficiency had dramatically worse outcomes than those with adequate levels.
Meta-analyses pooling data from dozens of observational studies found that vitamin D deficiency (under 20 ng/mL) was associated with roughly 80% higher hospitalization risk, 3-4 times higher ICU admission rates, and 2-3 times higher mortality. A 2021 meta-analysis published in Nutrients examining 54 studies found a clear dose-response relationship: progressively higher vitamin D levels correlated with progressively better outcomes up to approximately 50 ng/mL.
This correlation doesn’t prove that vitamin D supplementation prevents COVID or that giving vitamin D to already-sick patients would change outcomes. Association isn’t causation, and sick, elderly, or institutionalized patients often have lower vitamin D levels for reasons unrelated to immune function. But the pandemic highlighted what immunologists had long understood: vitamin D is crucial for immune system regulation, affecting how your body fights infections, regulates inflammation, and maintains immune balance.
The COVID data renewed attention to decades of research on vitamin D and immune function, with implications extending far beyond any single virus.
How Vitamin D Regulates Immune Function
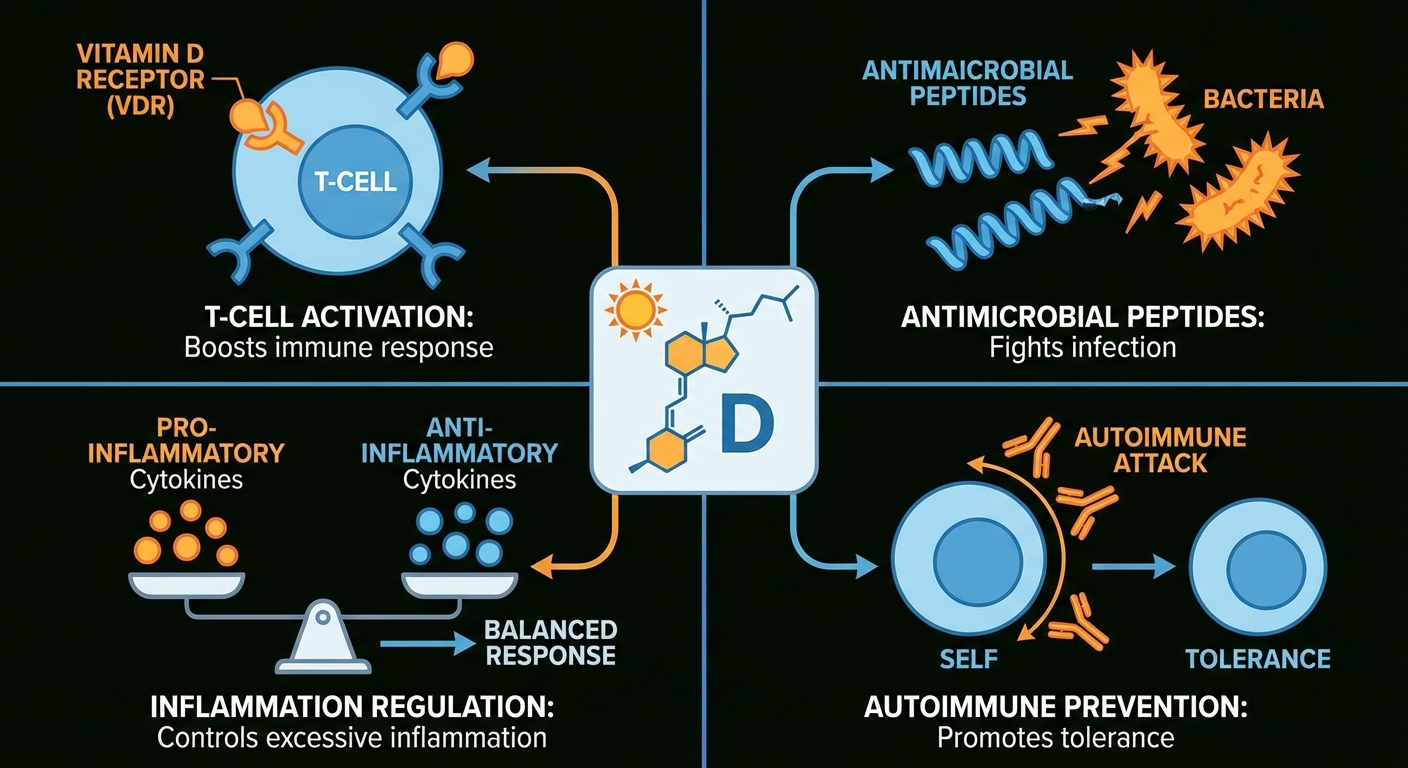
Vitamin D performs multiple critical functions in immune regulation that go far beyond its well-known role in bone health. Virtually every immune cell type expresses vitamin D receptors, meaning they’re designed to respond to vitamin D signaling. When vitamin D levels are inadequate, these cells don’t function optimally.
T-cell activation requires vitamin D. T-cells are the coordinators of your adaptive immune system, directing responses to specific pathogens and maintaining immunological memory. Research published in Nature Immunology demonstrated that T-cells have vitamin D receptors on their surfaces, and without adequate vitamin D, they remain in a naive, dormant state even when they should be responding to threats. This represents a fundamental impairment of adaptive immunity.
Antimicrobial peptide production depends on vitamin D status. The vitamin induces production of cathelicidin and defensins, proteins that directly kill bacteria and viruses by disrupting their membranes. These peptides function as your body’s natural antibiotics, providing first-line defense against pathogens before the adaptive immune system engages. A 2006 study in Science showed that vitamin D was essential for this antimicrobial response, explaining why people with deficiency are more susceptible to infections like tuberculosis.
Inflammation regulation represents another critical function. Vitamin D modulates the inflammatory response to prevent excessive inflammation while maintaining sufficient pathogen-fighting capacity. It shifts the immune system away from pro-inflammatory cytokines (like IL-6 and TNF-alpha, implicated in severe COVID-19) and toward a more balanced response. This helps explain why vitamin D deficiency is associated with cytokine storms and severe inflammatory responses to infection.
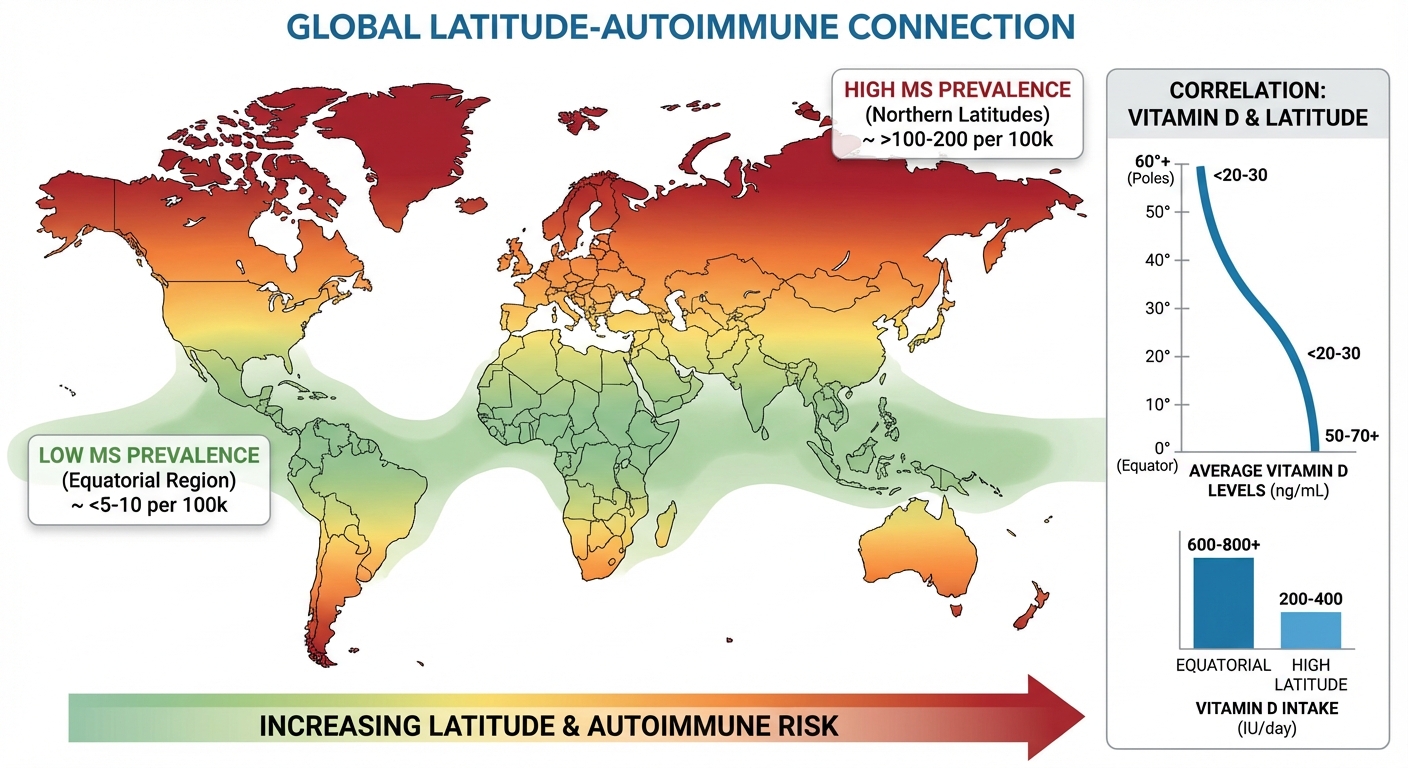
Autoimmune prevention appears to involve vitamin D as well. The vitamin helps maintain immune tolerance, preventing the immune system from mistakenly attacking the body’s own tissues. Geographic studies consistently show that autoimmune diseases including multiple sclerosis, type 1 diabetes, and rheumatoid arthritis become more common further from the equator, where sun exposure and vitamin D production decrease.
The COVID-19 Observational Evidence
The pandemic provided unprecedented opportunity to observe how nutritional status influences viral outcomes at massive scale. As researchers analyzed patient data, the vitamin D signal appeared repeatedly and consistently.
A 2020 study published in JAMA Network Open found that COVID-19 patients who were vitamin D deficient were 77% more likely to test positive for the virus. A 2021 meta-analysis in The Lancet Diabetes & Endocrinology found that low vitamin D status was associated with significantly increased risk of severe COVID-19 outcomes. The pattern held across different countries, healthcare systems, and demographic groups.
The dose-response pattern was particularly compelling. Studies didn’t just show that “deficient is bad”; they showed that progressively higher levels correlated with progressively better outcomes. Patients with levels above 40 ng/mL had the best outcomes. Those between 30-40 ng/mL had intermediate outcomes. Those below 20 ng/mL had the worst. This gradient suggests a real biological relationship rather than just a marker of overall health.
Supplementation trials during the pandemic produced mixed results, which deserves honest acknowledgment. Some studies, like a Spanish trial giving high-dose calcifediol (activated vitamin D) to hospitalized patients, showed significant reductions in ICU admission. Others showed minimal benefit from supplementation in acute illness. The pattern suggested that chronic adequate vitamin D status might be protective, but giving high doses to already-sick patients showed less benefit. Prevention appeared more effective than treatment.
Important caveats: Observational data cannot prove causation. Sick people might have lower vitamin D levels because they’re indoors more, eat poorly, or have conditions that impair vitamin D metabolism. Confounding factors like age, obesity, diabetes, and overall health status all influence both vitamin D levels and COVID-19 outcomes. The evidence is suggestive but not definitive for vitamin D as a direct protective factor against COVID-19.
Beyond COVID: The Broader Respiratory Infection Evidence
The pandemic brought attention to vitamin D’s immune role, but research on respiratory infections predates COVID-19 by decades. This longer evidence base provides context for interpreting the pandemic findings.
A landmark 2017 meta-analysis published in the BMJ analyzed individual patient data from 25 randomized controlled trials involving over 11,000 participants. Vitamin D supplementation reduced the risk of acute respiratory tract infection by 12% overall. But the effect was dramatically stronger in people who were deficient at baseline: those with levels below 20 ng/mL saw a 70% reduction in respiratory infections with supplementation. This threshold effect, where supplementation helps the deficient dramatically but does little for the replete, appears consistently in vitamin D research.
Seasonal patterns provide additional suggestive evidence. Vitamin D levels drop during winter months when sun exposure is limited. Flu and cold incidence increases during these same months. This correlation doesn’t prove causation (indoor crowding and dry air also increase in winter), but the timing aligns with what you’d expect if vitamin D contributed to respiratory defense.
Tuberculosis provides perhaps the strongest historical connection. Before antibiotics, TB treatment relied heavily on sunlight exposure (heliotherapy), with sanitariums specifically designed to maximize patients’ sun exposure. Modern research shows that vitamin D is essential for activating the antimicrobial response against tuberculosis bacteria, validating the historical practice.
For people who are deficient, correcting the deficiency with supplementation clearly reduces infection frequency and severity. For people who are already adequate, additional supplementation provides minimal additional benefit. This is consistent with vitamin D functioning as a necessary cofactor that limits immune function when absent but doesn’t boost it beyond normal when present in excess.
Autoimmune Disease Connections
A healthy immune system must balance aggression against pathogens with tolerance of self-tissues. When this discrimination fails, autoimmune diseases arise. Vitamin D plays a crucial role in maintaining this balance, acting as an immunomodulator rather than simply an immune booster.
Geographic distribution of autoimmune diseases provided the first clue. Multiple sclerosis, type 1 diabetes, and inflammatory bowel disease all become more common at higher latitudes, where sun exposure and vitamin D production decrease. MS rates, for example, are roughly twice as high in northern Europe and Canada as they are near the equator. While other factors differ by latitude (infections, diet, genetics of population), the vitamin D hypothesis remains one of the leading explanations.
Observational studies consistently find associations between low vitamin D levels and autoimmune disease risk. People with MS, type 1 diabetes, rheumatoid arthritis, inflammatory bowel disease, and psoriasis tend to have lower vitamin D levels than healthy controls. The causality question remains: does low vitamin D contribute to autoimmune development, or does autoimmune disease lead to behaviors (staying indoors, dietary changes) that reduce vitamin D?
Supplementation for existing autoimmune disease shows mixed results. Some studies show benefit, others show minimal effect. The pattern again suggests that maintaining adequate vitamin D might help prevent autoimmune disease development, but supplementation after disease is established has less impact. The 2022 VITAL study, a large randomized trial, found that vitamin D supplementation reduced autoimmune disease incidence by 22% over 5 years compared to placebo, providing some of the strongest evidence for a preventive role.
Optimal Vitamin D Levels for Immune Function
A major source of confusion is the difference between preventing deficiency disease (rickets, osteomalacia) and optimizing immune function. The reference ranges on standard lab tests were established to prevent severe bone disease, not to support peak immune function.
The bone health threshold of 20 ng/mL, established by the Institute of Medicine, prevents rickets and maintains basic calcium metabolism. Many people with levels between 20-30 ng/mL are told they’re “normal” when they may be suboptimal for immune function.
The immune optimization range of 40-60 ng/mL is recommended by many immunologists, integrative medicine practitioners, and researchers focused on vitamin D beyond bone health. This higher target is based on studies showing improved immune outcomes at these levels and on evolutionary reasoning, humans who evolved outdoors near the equator likely maintained levels in this range naturally.
The toxicity threshold of approximately 100 ng/mL is rarely reached with standard supplementation. True vitamin D toxicity, causing hypercalcemia, nausea, and kidney problems, typically requires sustained intake of 10,000+ IU daily for months or megadoses like 50,000+ IU weekly long-term.
The practical implication: If your lab report says “normal” at 22 ng/mL, you’re not deficient enough to develop rickets, but you may be suboptimal for immune function. For immune support specifically, aiming for 40-50 ng/mL appears reasonable based on current evidence, though not universally agreed upon by all medical organizations.
Getting to Optimal Levels
Achieving adequate vitamin D status involves three potential sources: sun exposure, food, and supplementation. For most modern humans, supplementation is necessary because lifestyle and geography have severed the evolutionary connection to sufficient sun exposure.
Sun exposure produces vitamin D when UVB rays hit exposed skin. The amount needed varies dramatically by latitude, season, skin tone, and time of day. General guidelines suggest 10-30 minutes of midday sun on arms and legs several times weekly, but people with darker skin may need 3-5 times longer exposure. Windows block UVB, and sunscreen reduces production by 95%+.
Food sources are limited. Fatty fish provides 400-1,000 IU per serving. Fortified milk offers about 100 IU per cup. Egg yolks contain roughly 40 IU each. UV-exposed mushrooms provide variable amounts. Getting adequate vitamin D from food alone is mathematically difficult for most people.
Supplementation is the most reliable method for most people. General guidelines for achieving 40-60 ng/mL levels:
| Starting Level | Daily Dose | Retest Timeline |
|---|---|---|
| Under 20 ng/mL | 5,000-10,000 IU | 8-12 weeks |
| 20-30 ng/mL | 2,000-5,000 IU | 8-12 weeks |
| 30-40 ng/mL | 1,000-2,000 IU | 12 weeks |
| 40-60 ng/mL | 1,000-2,000 IU (maintenance) | Annually |
Form matters: Vitamin D3 (cholecalciferol) is preferred over D2 (ergocalciferol). D3 is more effective at raising blood levels, as documented in our vitamin D optimization guide.
Cofactors are essential: Vitamin D requires magnesium for conversion to active form. Magnesium deficiency reduces vitamin D effectiveness and can cause side effects when supplementing. Vitamin K2 helps direct calcium into bones rather than soft tissues. Taking high-dose vitamin D without adequate magnesium is less effective and potentially problematic.
Testing: The Only Way to Know Your Status
Symptoms of vitamin D deficiency are non-specific (fatigue, weakness, mood changes) and overlap with many other conditions. The only way to know your actual status is blood testing.
The test to request is 25-hydroxyvitamin D (25(OH)D), which measures your body’s storage form. Don’t confuse this with 1,25-dihydroxyvitamin D, which measures the active hormone form and doesn’t accurately reflect overall status.
Testing frequency: Baseline test before starting supplementation, follow-up test 8-12 weeks after starting a new dose (this is how long it takes for levels to stabilize), and maintenance testing annually for most people. Those at higher risk (northern latitudes, darker skin, indoor lifestyle, obesity) may benefit from testing twice yearly.
Cost and access: The 25(OH)D test typically costs $30-50 and is available through most primary care providers. Direct-to-consumer lab testing is also available if your provider is reluctant to order it.
Special Populations With Higher Needs
Certain groups face significantly greater challenges maintaining adequate vitamin D levels:
Older adults have reduced skin synthesis capacity (a 70-year-old produces roughly 25% as much vitamin D from sun exposure as a 20-year-old) and often have reduced kidney conversion to active form. Higher supplementation is typically needed.
People with darker skin have melanin that naturally blocks UVB radiation. While this protects against skin cancer and sunburn, it also dramatically reduces vitamin D production, with some estimates suggesting 3-5 times more sun exposure is needed to produce equivalent vitamin D.
Obese individuals have vitamin D sequestered in fat tissue, making it less bioavailable. Studies suggest obese people may need 2-3 times higher supplementation to achieve the same blood levels.
Northern latitude residents experience months when the sun angle is too low to produce vitamin D regardless of time spent outside. Above roughly 37°N latitude (San Francisco to Philadelphia), vitamin D production is negligible from November through February.
Indoor workers and people who consistently avoid sun exposure receive minimal UV exposure regardless of latitude or season.
These populations benefit most from supplementation and should prioritize testing to guide dosing.
The Bottom Line
Vitamin D is crucial for immune function. It’s required for T-cell activation, antimicrobial peptide production, inflammation regulation, and maintenance of immune tolerance. Deficiency impairs your ability to fight infections and regulate inflammatory responses.
COVID-19 research highlighted these connections dramatically, but the evidence extends far beyond any single virus. Decades of research show that vitamin D deficiency increases susceptibility to respiratory infections, and correcting deficiency with supplementation reduces infection risk by up to 70% in deficient populations.
For immune support, target blood levels of 40-50 ng/mL appear reasonable based on current evidence, though this is higher than the 20 ng/mL threshold established for bone health alone. Most people need supplementation to achieve these levels, particularly in winter or if they have risk factors for deficiency.
Next Steps:
- Get a 25-hydroxyvitamin D blood test to establish your baseline
- Supplement based on your current level to reach 40-50 ng/mL
- Ensure adequate magnesium intake (320-420mg daily) to support vitamin D metabolism
- Retest in 8-12 weeks to verify your supplementation is working
- Maintain with ongoing supplementation, especially during winter months
Sources: JAMA Network Open 2020 COVID vitamin D study, BMJ 2017 respiratory infection meta-analysis, Nature Immunology T-cell activation study, Science 2006 antimicrobial peptide study, Nutrients 2021 COVID meta-analysis, The Lancet Diabetes & Endocrinology vitamin D outcomes study, VITAL autoimmune disease trial 2022.