Your doctor says your vitamin D level is “normal” at 22 ng/mL. You’re taking the recommended 600 IU daily. On paper, everything looks fine. Yet you’re still catching every cold that circulates through your office, your energy crashes by 3 PM, and last winter’s seasonal mood dip felt worse than ever. The disconnect between “adequate” vitamin D status and optimal health outcomes is one of the most significant gaps between outdated guidelines and current research.
Vitamin D deficiency is arguably the most common nutritional deficiency in the industrialized world, with estimates suggesting over 40% of Americans are deficient. That number climbs higher in northern latitudes, among people with darker skin, those who work indoors, and anyone who diligently wears sunscreen. This widespread insufficiency has significant implications for public health, affecting everything from susceptibility to viral infections to long-term bone density, muscle function, and mood regulation.
For decades, the Recommended Daily Allowance (RDA) was set at a modest 600 IU for adults under 70, increased to 800 IU for older adults. However, these recommendations were established primarily to prevent rickets and osteomalacia, the severe deficiency diseases. They were never designed to optimize immune function, athletic performance, or the hundreds of other physiological processes that vitamin D influences. The emerging consensus from endocrinology, immunology, and metabolic research suggests these numbers are barely adequate for disease prevention, let alone biological optimization.
Understanding Blood Level Testing: Normal vs. Optimal
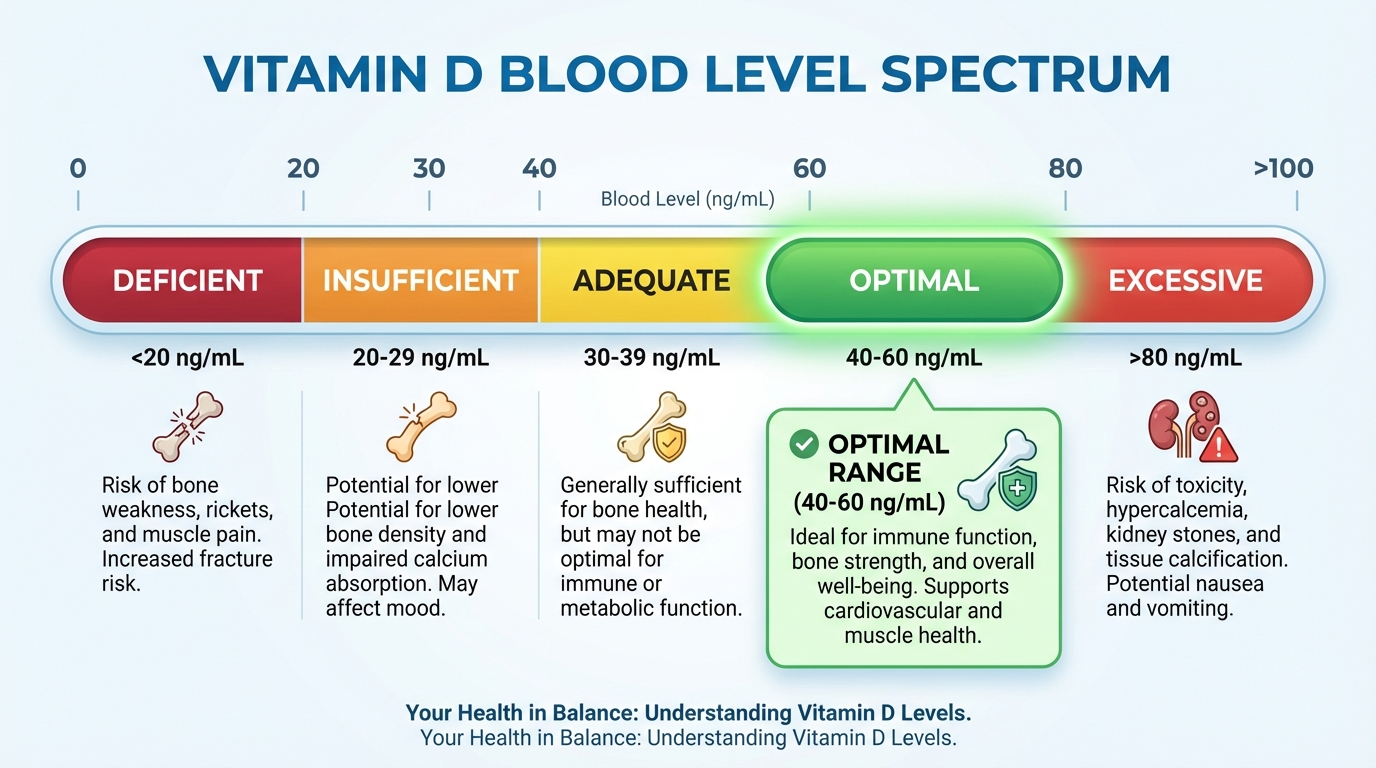
When you get a vitamin D blood test (specifically, 25-hydroxyvitamin D or 25(OH)D), the lab report typically lists a “normal” reference range of 20-100 ng/mL. This range is so wide that it includes levels many researchers now consider functionally deficient alongside levels that approach toxicity risk. A result of 22 ng/mL and 60 ng/mL are both “normal” by this definition, yet they represent vastly different physiological states.
The Endocrine Society defines vitamin D deficiency as levels below 20 ng/mL and insufficiency as 21-29 ng/mL. However, functional medicine practitioners and recent research point to a more nuanced target range. Levels below 30 ng/mL are now widely considered insufficient for bone maintenance, let alone the more complex metabolic functions vitamin D supports. A 2023 meta-analysis published in Nutrients examining 14 randomized controlled trials found that the threshold for optimal immune function appears to be approximately 40 ng/mL, with benefits plateauing around 60 ng/mL.
Target blood levels by health goal:
- Preventing deficiency diseases: 20+ ng/mL (bare minimum)
- Bone health maintenance: 30+ ng/mL
- Optimal immune function: 40-60 ng/mL
- Upper limit before diminishing returns: 60 ng/mL
- Toxicity risk threshold: 100+ ng/mL (with prolonged exposure)
Reaching the 40-60 ng/mL sweet spot typically requires significantly higher intake than the standard RDA. Most adults require 2,000 to 5,000 IU daily to achieve and maintain these levels, with some individuals needing even more depending on body composition, absorption efficiency, and sun exposure. Obesity, in particular, dramatically increases vitamin D requirements because the fat-soluble vitamin gets sequestered in adipose tissue and becomes less bioavailable.
The D2 vs. D3 Question: Form Matters Significantly
The form of vitamin D you choose matters more than many people realize. Vitamin D2 (ergocalciferol) is derived from plant and fungal sources and is often the form prescribed in high-dose pharmaceutical preparations. Vitamin D3 (cholecalciferol) is derived from animal sources (typically lanolin from sheep’s wool) or lichen and is chemically identical to the vitamin your skin produces when exposed to UVB radiation.
Research consistently shows that D3 is significantly more effective at raising and maintaining blood levels compared to D2. A 2012 meta-analysis in the American Journal of Clinical Nutrition found that D3 was approximately 87% more potent than D2 at raising serum 25(OH)D levels. The difference appears to stem from D3’s greater affinity for vitamin D-binding protein in the blood and its more efficient conversion to the active hormone form.
This distinction has practical implications for supplementation strategy. When choosing a supplement, verify that you’re getting D3 (cholecalciferol), not D2 (ergocalciferol). If you’ve been prescribed high-dose D2 by a physician to correct a deficiency, this may be appropriate for short-term repletion, but most experts recommend transitioning to D3 for maintenance dosing. Vegans and vegetarians can now find D3 derived from lichen, which provides the more bioavailable form without animal-derived ingredients.
The Critical Co-Factors: Why Vitamin D Alone Isn’t Enough
Vitamin D supplementation doesn’t occur in a biochemical vacuum. The vitamin requires several co-factors to be properly absorbed, metabolized, and utilized. Taking high-dose vitamin D without addressing these co-factors can be ineffective at best and potentially problematic at worst.
The Magnesium Requirement
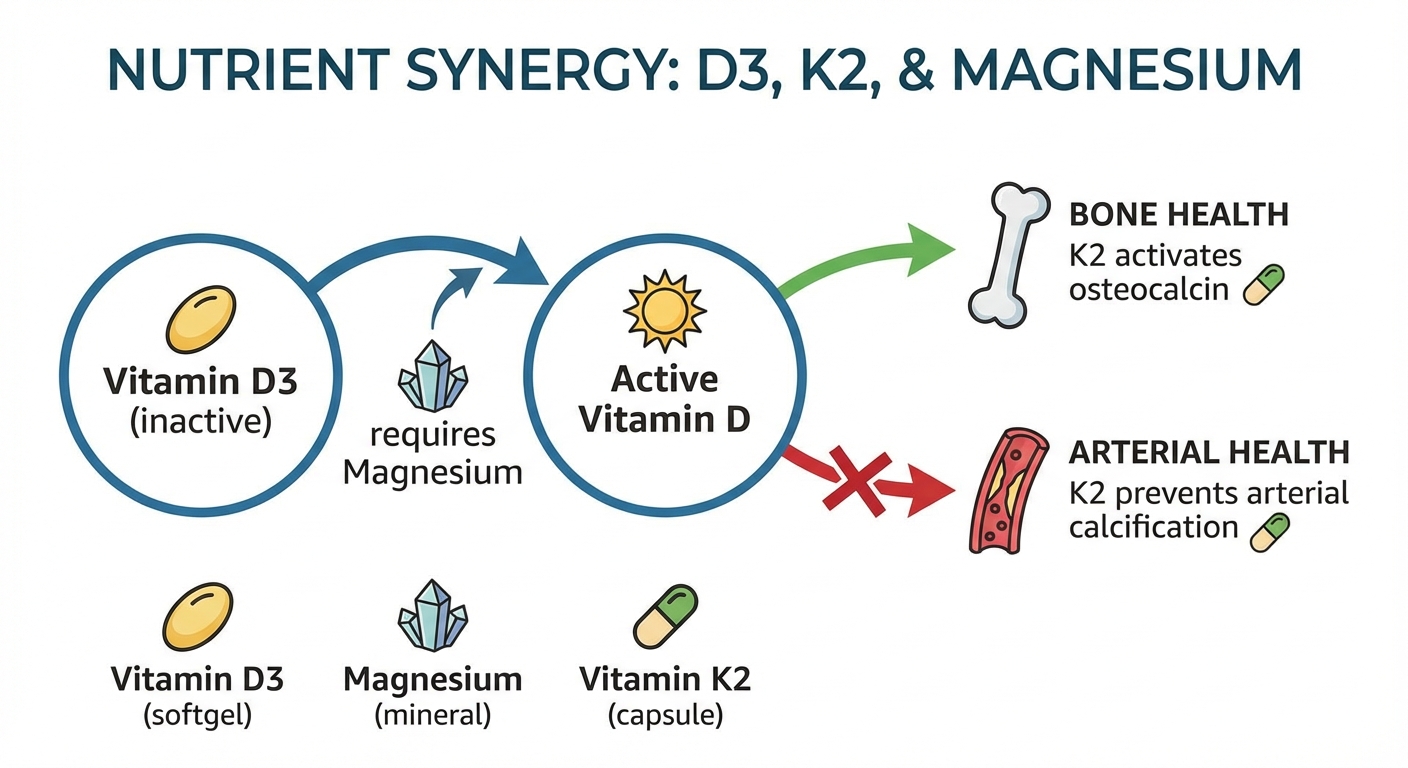
Vitamin D supplements are biologically inactive when you swallow them. To become useful, they must be converted through a two-step process: first by the liver into 25-hydroxyvitamin D (the storage form measured in blood tests), then by the kidneys into 1,25-dihydroxyvitamin D (calcitriol, the active hormone form). Both conversion steps are entirely magnesium-dependent.
If you’re deficient in magnesium, which approximately 50% of the American population is, taking high-dose vitamin D can actually deplete your magnesium stores further as the body works to process the vitamin D. This explains why some people experience headaches, anxiety, muscle cramps, or heart palpitations when they start a vitamin D regimen. It’s often a masked magnesium deficiency being exacerbated by the metabolic demand of vitamin D conversion.
The research connecting these two nutrients is compelling. A 2018 study published in the Journal of the American Osteopathic Association found that vitamin D supplementation was ineffective at correcting deficiency in participants who were also magnesium-deficient. Understanding the different forms of magnesium and ensuring adequate intake (320-420mg daily for adults) is essential before pursuing aggressive vitamin D supplementation.
The Vitamin K2 Connection: Directing Calcium Traffic
One of the most important advances in vitamin D research is understanding its relationship with vitamin K2. Vitamin D increases calcium absorption from the gut, which is generally beneficial for bone health. However, without adequate vitamin K2, that absorbed calcium can be misdirected. Instead of depositing in your bones where it’s needed, it can accumulate in your arteries, heart valves, or kidneys, contributing to calcification.
Vitamin K2 acts as the traffic controller for this calcium. It activates two critical proteins: osteocalcin (which pulls calcium into bones) and matrix GLA protein (MGP), which prevents calcium from depositing in soft tissues like blood vessels. Without adequate K2, these proteins remain inactive, and calcium goes wherever blood flow takes it rather than where the body needs it.
The synergy between D3 and K2 has been demonstrated in multiple studies. A 2017 study in Clinical Interventional Aging found that the combination of vitamin D3 and K2 (as MK-7, the most bioavailable form) improved bone mineral density more effectively than either nutrient alone. The researchers noted that the combination appeared to both increase calcium absorption (D3’s effect) and ensure proper calcium utilization (K2’s effect).
Practical recommendation: When supplementing with vitamin D3 at doses above 2,000 IU daily, include vitamin K2 (as MK-7) at 100-200mcg daily. Many manufacturers now produce combination supplements specifically because of this synergy.
Absorption Optimization: Timing and Context Matter
Even with the right form and co-factors, vitamin D absorption varies significantly based on when and how you take it. As a fat-soluble vitamin, D3 requires dietary fat for optimal absorption. Taking your supplement with a glass of water on an empty stomach may result in absorbing as little as 30% of the dose.
A 2015 study in the Journal of the Academy of Nutrition and Dietetics found that taking vitamin D with a fat-containing meal increased absorption by approximately 50% compared to taking it without food. The type of fat matters less than the presence of fat itself. Whether it comes from avocado, olive oil, eggs, or nuts, consuming 10-15 grams of fat alongside your vitamin D supplement significantly improves bioavailability.
Timing recommendations:
- Take with your largest meal of the day (typically lunch or dinner, which usually contains adequate fat)
- Morning vs. evening: Some evidence suggests morning dosing may be preferable, as vitamin D can compete with melatonin pathways. If you notice sleep disruption after starting supplementation, try moving your dose to earlier in the day.
- Consistency matters more than perfect timing: A regular daily dose produces more stable blood levels than sporadic high doses.
Dosing Protocols: From Deficiency to Optimization
The appropriate vitamin D dose depends heavily on your starting blood level, body composition, absorption efficiency, and health goals. The one-size-fits-all RDA of 600 IU reflects the minimum needed to prevent deficiency in the average healthy adult, not the amount required to reach optimal levels.
Dosing guidelines based on current blood levels:
| Current Level | Goal | Suggested Daily Dose | Retest Timeline |
|---|---|---|---|
| Under 20 ng/mL (deficient) | Repletion to 40+ | 5,000-10,000 IU | 8-12 weeks |
| 20-29 ng/mL (insufficient) | Optimization to 40-60 | 4,000-5,000 IU | 8-12 weeks |
| 30-39 ng/mL (adequate) | Optimization to 50+ | 2,000-4,000 IU | 12 weeks |
| 40-60 ng/mL (optimal) | Maintenance | 1,000-2,000 IU | Annually |
Important caveats: These are general guidelines, not prescriptions. Individual responses to supplementation vary significantly based on genetics, body composition, and baseline status. Obese individuals typically require 2-3x higher doses to achieve the same blood level increases as normal-weight individuals because vitamin D is sequestered in fat tissue.
Toxicity considerations: Vitamin D toxicity is rare but possible with sustained high-dose supplementation (typically 50,000+ IU daily for months). Symptoms include hypercalcemia, nausea, vomiting, weakness, and kidney problems. The Endocrine Society considers doses up to 4,000 IU daily safe for healthy adults without monitoring, but doses above this level warrant periodic blood testing to ensure levels stay below 100 ng/mL.
Special Populations: Who Needs More?
Certain populations have significantly higher vitamin D requirements or face greater challenges maintaining adequate levels:
Darker skin tones: Melanin reduces the skin’s ability to produce vitamin D from sunlight by up to 90%. People with darker skin living in northern latitudes often require substantially higher supplementation to maintain adequate levels.
Older adults: Skin synthesis efficiency decreases with age, and kidney conversion to the active form becomes less efficient. Adults over 70 may need 1,000-2,000 IU daily just to maintain adequate (not optimal) levels.
Obese individuals: Body fat sequesters vitamin D, making it less bioavailable. Studies suggest obese individuals may need 2-3 times higher doses to achieve equivalent blood level increases.
Northern latitude residents: Above approximately 37°N latitude (roughly the line from San Francisco to Philadelphia), UVB radiation is insufficient to produce vitamin D in the skin for 4-6 months of the year. Winter vitamin optimization strategies become particularly important for these populations.
Indoor workers: Those who spend the majority of daylight hours indoors receive minimal UVB exposure regardless of latitude or season.
Testing Protocol: When and How Often
Blood testing is the only way to know your actual vitamin D status and whether your supplementation protocol is working. Relying on symptoms alone is unreliable because deficiency symptoms (fatigue, muscle weakness, mood changes) overlap with many other conditions.
Testing recommendations:
- Baseline test: Before starting or changing supplementation
- Follow-up test: 8-12 weeks after starting a new dose (this is approximately how long it takes for blood levels to stabilize on a new regimen)
- Maintenance testing: Annually for most people, or twice yearly if you live in northern latitudes (test in late winter when levels are lowest and late summer when levels are highest)
Request the 25-hydroxyvitamin D test specifically, not the 1,25-dihydroxyvitamin D test. The 25(OH)D test measures your body’s storage form and accurately reflects your vitamin D status. The 1,25 test measures the active hormone form, which the body tightly regulates and doesn’t reflect overall sufficiency.
Many primary care physicians will order this test as part of routine bloodwork if you request it. Direct-to-consumer lab testing is also available if your provider is reluctant or if you want more frequent monitoring than insurance typically covers.
The Bottom Line
Vitamin D is far more than a bone-health nutrient. It functions as a hormone precursor that influences the expression of hundreds of genes involved in immune function, muscle maintenance, mood regulation, and metabolic health. The old RDA of 600 IU represents the bare minimum to prevent severe deficiency diseases, not the amount required for optimal health outcomes.
The emerging research consensus points to several key principles: target blood levels of 40-60 ng/mL for optimal function (not just 20+ to avoid deficiency); use vitamin D3, not D2; always pair supplementation with adequate magnesium and vitamin K2; take with fat-containing meals for maximum absorption; and test periodically to verify that your protocol is working.
Next Steps:
- Request a 25-hydroxyvitamin D blood test to establish your baseline
- Calculate your target dose based on current levels (use the table above as a starting point)
- Choose a quality D3 supplement, ideally combined with K2 (MK-7)
- Ensure adequate magnesium intake (320-420mg daily) before high-dose D3
- Take with your largest meal for optimal absorption
- Retest in 8-12 weeks to verify your protocol is working
Sources: American Journal of Clinical Nutrition 2012 D2 vs D3 meta-analysis, Nutrients 2023 immune function meta-analysis, Journal of the American Osteopathic Association 2018 magnesium-vitamin D study, Clinical Interventional Aging 2017 D3+K2 bone study, Journal of the Academy of Nutrition and Dietetics 2015 absorption study, Endocrine Society vitamin D guidelines.