Imagine telling your employer you need to leave work early every weekday for the next six weeks. Not for vacation. Not for a temporary project. For a medical treatment that insurance might or might not cover, that requires driving to a clinic, sitting in a chair for 20 to 40 minutes while a magnetic coil pulses against your skull, and then driving home, five days a week, for a month and a half. For many people with treatment-resistant depression, this is what accessing transcranial magnetic stimulation (TMS) actually looks like. It’s not that the treatment doesn’t work. Standard TMS produces symptom improvement in 60 to 70% of patients and full remission in 25 to 35%. The problem is that the schedule makes it functionally inaccessible for a significant portion of the people who need it most.
A new study from UCLA, published in the Journal of Affective Disorders in February 2026, suggests the timeline could shrink dramatically. Researchers found that patients who received five TMS sessions per day over five consecutive days experienced symptom relief comparable to those who followed the traditional six-week schedule. Some patients who showed little immediate improvement after the compressed treatment went on to experience a 36% average drop in depression scores when reassessed two to four weeks later. The findings are not just a scheduling convenience. They point toward a fundamentally different model for how brain stimulation therapy could reach the millions of Americans living with depression that hasn’t responded to medication.
How TMS Rewires the Depressed Brain
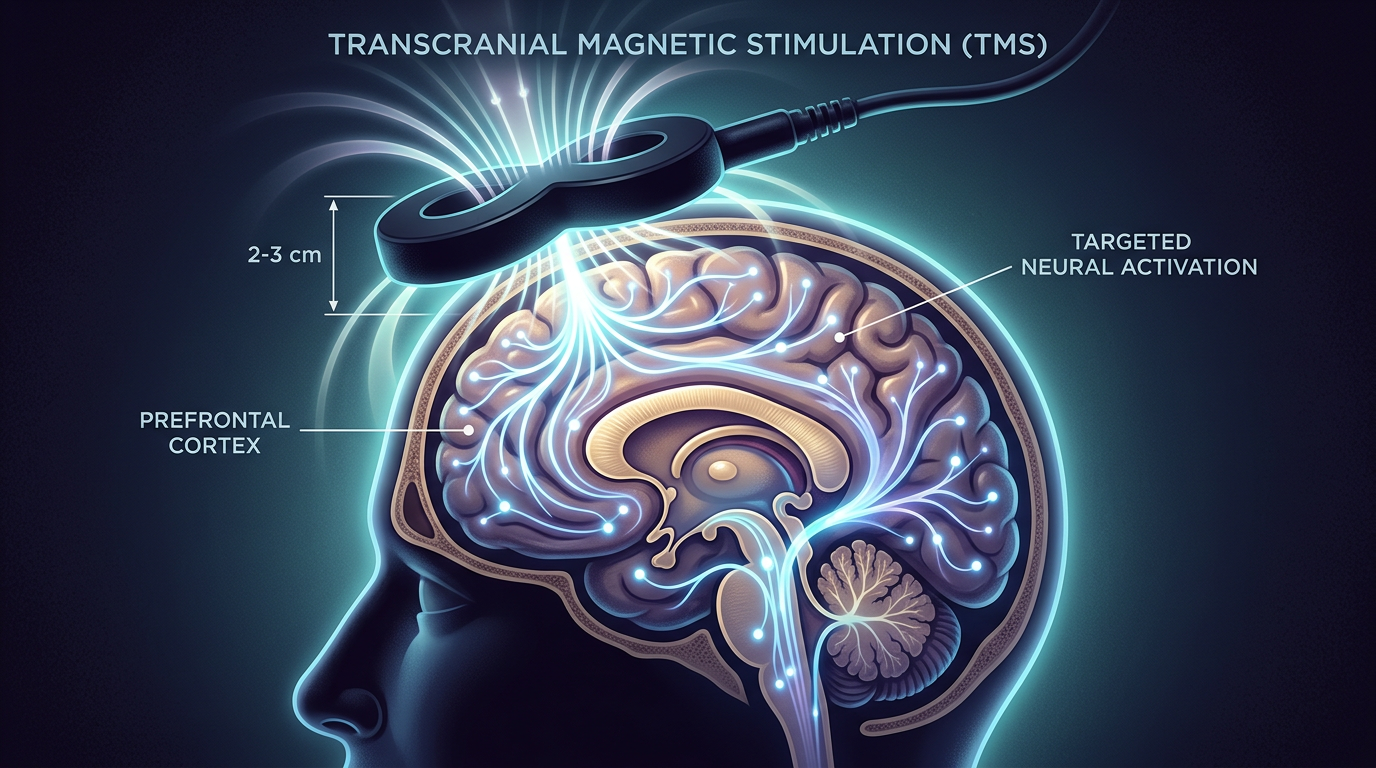
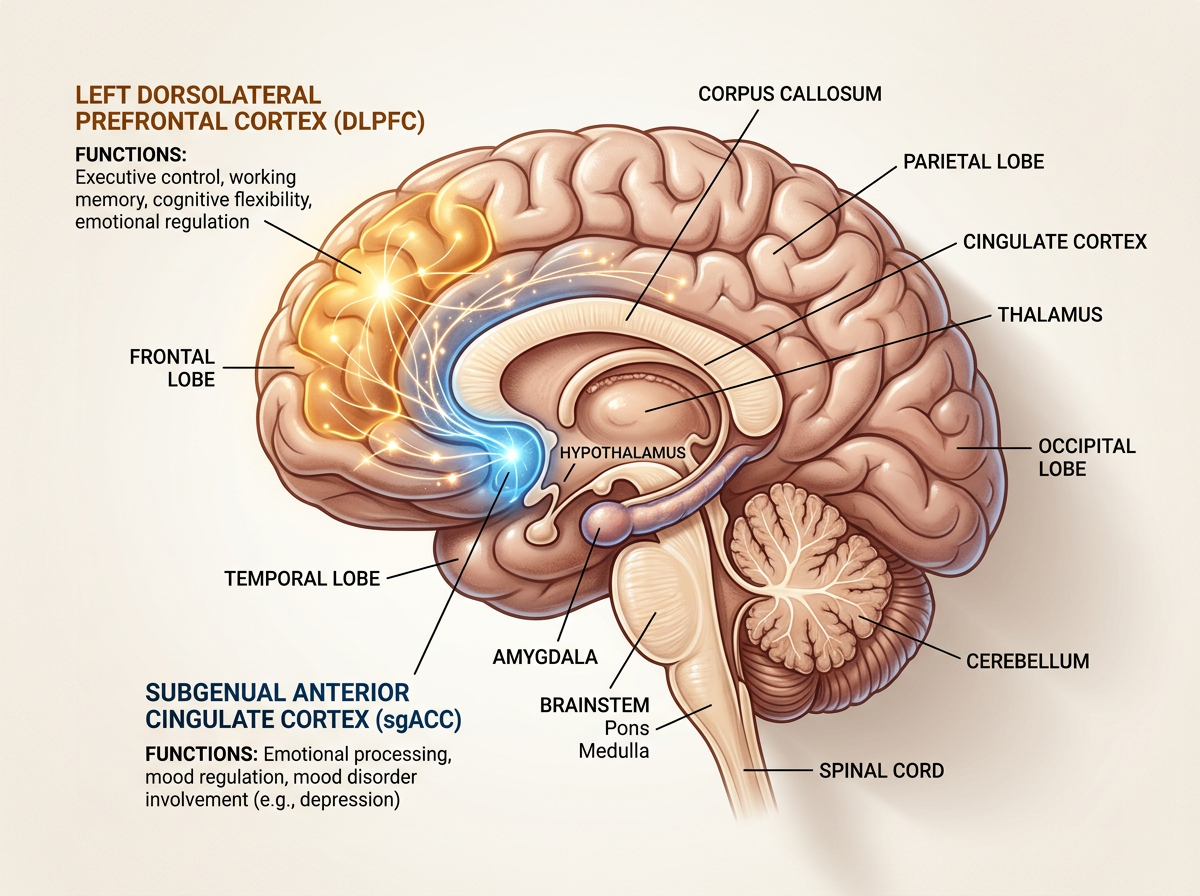
To understand why compressing TMS into five days might work, you first need to understand what the treatment does at a neurological level. TMS uses focused magnetic pulses to stimulate specific regions of the brain, most commonly the left dorsolateral prefrontal cortex (DLPFC). This area, located just behind your left temple, is consistently underactive in people with major depression. Brain imaging studies show reduced blood flow, lower metabolic activity, and weakened connections between the DLPFC and deeper emotional processing centers.
The DLPFC doesn’t operate in isolation. It connects to the subgenual anterior cingulate cortex (sgACC), a small but influential region buried deep in the brain’s midline that acts as a hub for negative emotional processing. In healthy brains, the DLPFC exerts a kind of top-down regulatory control over the sgACC, keeping negative emotional responses in check. In depressed brains, this regulatory connection weakens. The sgACC becomes overactive, generating persistent negative mood states that the weakened prefrontal cortex can’t suppress. Think of it as a volume knob for emotional pain that’s been turned up, with the part of the brain responsible for turning it down running at reduced power.
When TMS delivers repetitive magnetic pulses to the DLPFC, it triggers a cascade of neuroplastic changes. Neurons in the stimulated area fire more frequently, strengthening synaptic connections and increasing the release of neurotransmitters including serotonin, dopamine, and norepinephrine. Over time, the connection between the DLPFC and the sgACC strengthens, restoring the prefrontal cortex’s ability to regulate emotional responses. The process also appears to promote the release of brain-derived neurotrophic factor (BDNF), a protein that supports the growth and survival of neurons and is often depleted in people with depression.
The standard protocol spaces this stimulation across 30 sessions over six weeks, delivering one session per day. The rationale has traditionally been that neuroplastic changes need time to consolidate between sessions, similar to how muscles need rest days between strength training workouts. The UCLA study challenges that assumption by asking a simple question: what if the brain can handle, and benefit from, a much more concentrated dose?
The UCLA Study: What Researchers Found
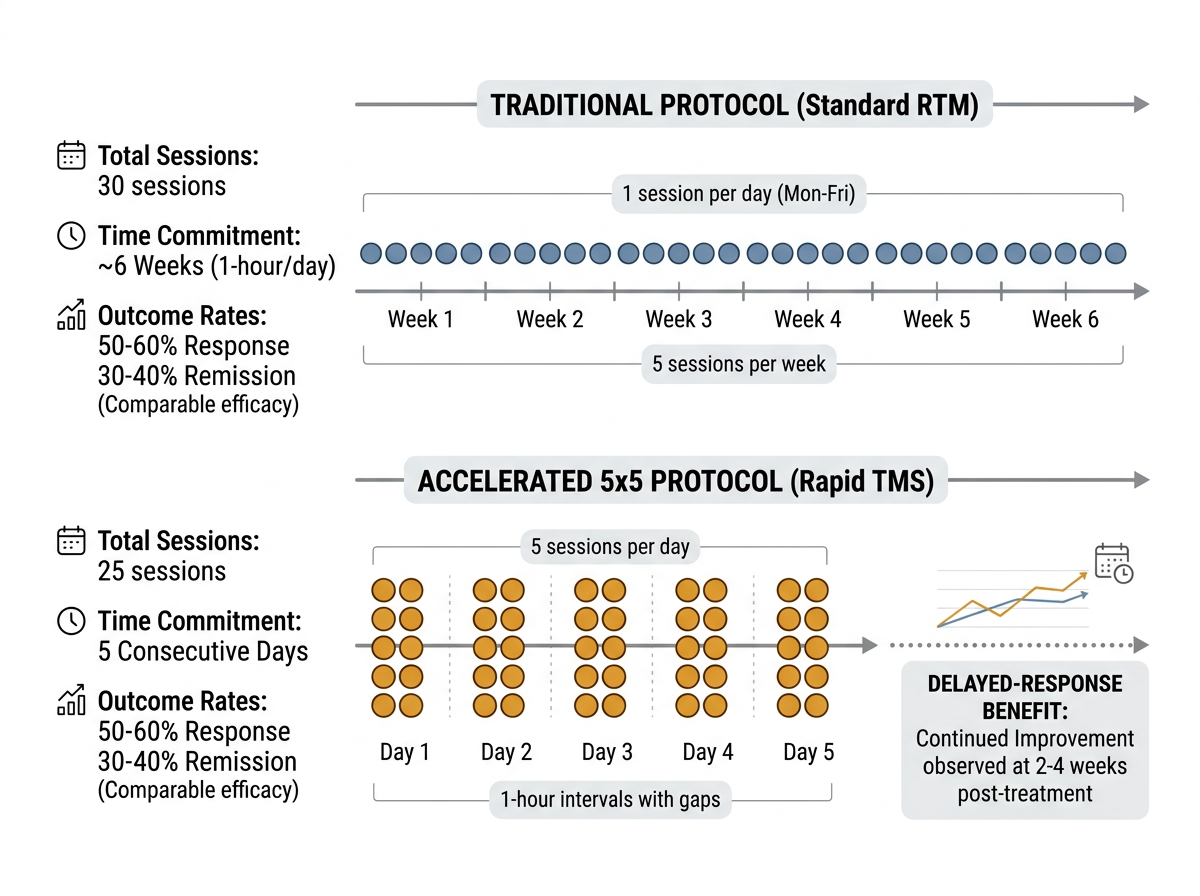
The study, led by Michael Apostol, a Ph.D. student at the UCLA Semel Institute for Neuroscience and Human Behavior, and supervised by Dr. Andrew Leuchter, a distinguished professor and director of the TMS Service in UCLA’s Department of Psychiatry and Biobehavioral Sciences, compared outcomes between two groups of patients with treatment-resistant depression. The first group of 135 patients received the conventional protocol: one TMS session per day, five days per week, for six weeks, totaling 30 sessions. The second group of 40 patients received what the researchers call the “5x5” protocol: five sessions per day for five consecutive days, totaling 25 sessions delivered in a single workweek.
Both groups experienced statistically significant reductions in depression symptoms, and the difference between the two groups was not statistically significant. In practical terms, patients who received one week of intensive treatment improved by roughly the same degree as patients who spent six weeks coming in daily. The finding held across multiple measures of depression severity, suggesting it wasn’t an artifact of any single assessment tool.
“For patients with treatment-resistant depression, getting to the clinic every weekday for at least six weeks can be a real obstacle,” Apostol noted. “What this study suggests is that we may be able to offer those same patients a path to meaningful relief in less than one week by condensing 25 TMS treatments over just five days.” The practical implications are enormous. A patient could take a single week of leave from work, complete an entire course of brain stimulation treatment, and return to normal life the following Monday. Compare that to the current standard, which requires six to eight weeks of daily clinic visits that disrupt employment, childcare, transportation, and daily routines.
One of the most intriguing findings involved the subset of patients in the accelerated group who didn’t show immediate improvement after their five days of treatment. Rather than concluding the compressed protocol had failed for these individuals, researchers followed up two to four weeks later and found that approximately one-third of these apparent non-responders had experienced substantial delayed improvement, with depression scores dropping by an average of 36%. “Some patients need to wait a few days or weeks to see benefit, and we encourage them not to give up too quickly,” Dr. Leuchter observed. This delayed-response pattern suggests that the neuroplastic changes initiated during the intensive treatment week continue developing after the sessions end, much like how physical exercise produces adaptation gains in the days following a workout rather than during the workout itself.
The Stanford SAINT Protocol: Context for a Growing Field
The UCLA study enters a field that Stanford researchers helped reshape with their own accelerated TMS protocol. The Stanford Accelerated Intelligent Neuromodulation Therapy (SAINT) protocol, which received FDA clearance in September 2022, compresses treatment into five days using a different approach: ten sessions per day, each lasting about ten minutes, spaced one hour apart, for a total of 50 sessions across the five-day period. SAINT also uses functional MRI brain imaging to identify the precise spot on each patient’s prefrontal cortex that has the strongest connection to the sgACC, allowing for individualized targeting rather than the standardized positioning used in most TMS protocols.
The results from Stanford’s clinical trials were striking. In a randomized, sham-controlled trial, 78% of participants who received SAINT achieved depression remission, compared to 13% in the placebo group. That remission rate far exceeds anything reported for standard TMS protocols. The precision targeting appears to matter: by identifying each patient’s optimal stimulation site through brain imaging, the protocol can deliver magnetic pulses to the exact neural pathway that needs strengthening, rather than relying on anatomical landmarks that may not correspond to the functional target in every individual.

The UCLA 5x5 protocol differs from SAINT in several important ways. It uses 25 total sessions rather than 50, does not require pre-treatment fMRI imaging, and relies on standard TMS coil positioning rather than individualized targeting. These differences make it potentially more accessible and less expensive than SAINT, which requires specialized imaging equipment and expertise that many clinics don’t have. The trade-off may be lower peak efficacy: SAINT’s 78% remission rate in controlled trials exceeds the remission rates typically seen with standard TMS approaches. But the UCLA study suggests that a simpler, less resource-intensive compressed protocol can still produce clinically meaningful results comparable to the traditional six-week schedule.
Both studies point in the same direction: the brain can tolerate and benefit from concentrated TMS exposure delivered over days rather than weeks. The precise optimal protocol, whether 25 sessions or 50, with or without fMRI guidance, using standard or theta-burst stimulation patterns, remains to be determined through larger randomized trials. But the era of requiring six to eight weeks for a course of TMS treatment appears to be ending.
What Five-Day Treatment Means for Access and Cost
The accessibility implications of compressed TMS schedules extend far beyond scheduling convenience. Standard TMS treatment typically costs between $6,000 and $12,000 for a full course, with individual sessions running $200 to $500 without insurance. Most major insurers now cover TMS for treatment-resistant depression, but coverage requires that patients have failed at least one (and often two or more) antidepressant medications. Even with insurance, copayments of $20 to $60 per session across 30 to 36 sessions add up to $600 to $2,160 in out-of-pocket costs, not counting transportation, lost wages, and childcare expenses accumulated over six weeks of daily appointments.
A five-day protocol could fundamentally change this economic calculus. The direct treatment cost would likely be lower, since clinics would deliver 25 sessions rather than 30, and the concentrated schedule reduces the overhead associated with intake, setup, and administrative processing spread across dozens of individual appointments. The indirect costs, those hidden expenses that insurance doesn’t cover, would shrink even more dramatically. One week of lost wages is a fraction of six weeks. One week of arranging childcare or transportation is manageable in a way that six to eight weeks is not. For patients in rural areas who might need to travel significant distances to reach a TMS-equipped clinic, the difference between six weeks of daily round trips and one intensive week with temporary lodging nearby could determine whether treatment is practically possible or effectively out of reach.
There is also a workforce dimension that rarely gets discussed. Depression is the leading cause of disability worldwide, and treatment-resistant depression, by definition, has not responded to standard antidepressant medications. Many of these patients are employed or seeking employment. Telling them to attend medical appointments five days a week for six weeks creates a tension between treating their illness and maintaining their livelihood. A single-week intensive treatment could be taken as a medical leave, similar to a minor surgical procedure, without the protracted disruption that current TMS scheduling demands. Employers, disability insurers, and workers’ compensation programs may all have reason to support the development and coverage of accelerated protocols.
The Delayed Response Puzzle
The finding that some patients in the accelerated group improved substantially in the weeks after treatment ended is one of the most scientifically interesting aspects of the UCLA study. It challenges a straightforward assumption about brain stimulation: that the benefits are proportional to what you feel immediately after the coil stops pulsing. Instead, the data suggest a more complex temporal dynamic, one where the treatment initiates biological processes that unfold on their own timeline.
This makes sense when you consider what TMS actually does at the cellular level. The magnetic pulses don’t directly fix anything. They trigger a cascade of neuroplastic events: synaptogenesis (the formation of new synaptic connections), changes in neurotransmitter receptor density, increases in BDNF expression, and gradual strengthening of long-range neural pathways between the prefrontal cortex and limbic structures. These processes take time. Just as a broken bone continues healing for weeks after the cast is set, the neural circuits activated by TMS continue reorganizing after the last session ends.
The delayed-response finding also carries practical importance for clinical decision-making. Under the current standard protocol, patients who aren’t responding after two or three weeks of daily sessions often face a difficult choice: continue the remaining weeks of treatment hoping for improvement, switch to a different approach, or give up on TMS entirely. If a subset of patients are delayed responders whose improvements appear on a lag, then premature abandonment of treatment could be denying them the benefit they would have experienced with patience. Dr. Leuchter’s advice that patients “not give up too quickly” may prove to be one of the study’s most important clinical takeaways, applicable to both accelerated and standard protocols.
The delayed response pattern also raises questions about the optimal timing for assessing TMS outcomes. Most clinical trials and insurance authorization processes evaluate TMS success immediately after the final session or within a few days. If one-third of accelerated-protocol patients show their peak improvement two to four weeks later, current assessment windows may be systematically underestimating the treatment’s true efficacy. Future studies will need to build in extended follow-up periods to capture the full trajectory of response, including these delayed gains.
What to Expect and What to Know Before Considering TMS
For anyone considering TMS, whether the standard or accelerated protocol, understanding the practical experience can reduce anxiety about the process. TMS is a noninvasive outpatient procedure that does not require anesthesia, sedation, or any recovery time. You remain fully awake and alert throughout. During a session, you sit in a reclining chair similar to what you’d find at a dentist’s office. A technician positions the TMS coil, a figure-eight shaped device about the size of a hand, against the left side of your head. When activated, the coil delivers rapid magnetic pulses that create a tapping sensation on the scalp. Most patients describe it as a repeated light knocking or clicking, noticeable but not painful. Each standard session lasts 20 to 40 minutes, though newer theta-burst stimulation protocols can deliver a full dose in as little as three minutes.
The most common side effect is mild scalp discomfort or headache at the stimulation site, which typically resolves within an hour and tends to diminish over the course of treatment as patients acclimate. Serious side effects are rare: the risk of seizure, the most significant concern, is approximately 1 in 30,000 sessions. There is no systemic sedation, no cognitive impairment, and no “recovery period” needed. Patients drive themselves to and from appointments and can return to work or daily activities immediately after each session. For the accelerated 5x5 protocol, the daily experience would be more intensive. Five sessions in a single day, with breaks between them, means spending several hours at the clinic rather than the typical 30 to 60 minutes. The UCLA study did not report significantly elevated side effects in the accelerated group compared to the standard group, which is encouraging, though the smaller sample size of 40 patients means that uncommon side effects may not have been captured. Anyone considering TMS should discuss the full range of treatment options with their psychiatrist or physician, including whether the accelerated or standard protocol is more appropriate for their specific clinical situation.
The UCLA study itself has meaningful limitations that should inform how we interpret its results. The most significant is that it was not a randomized controlled trial. Patients were not randomly assigned to the standard or accelerated group, meaning that differences between the groups beyond the treatment schedule itself could have influenced the outcomes. The accelerated group was also considerably smaller (40 patients versus 135), limiting the statistical power to detect differences between the two approaches. These are standard limitations in preliminary research, and the authors are transparent about them, but they mean the findings should be considered promising evidence rather than definitive proof.
Larger, randomized, controlled trials are the necessary next step. These studies would need to randomly assign patients to accelerated versus standard protocols, control for variables like depression severity and medication history, and follow patients for months after treatment to compare the durability of response between the two approaches. The delayed-response finding in particular needs replication in larger samples, since the one-third of accelerated patients who showed delayed improvement is a relatively small absolute number of individuals.
It is also worth noting that TMS, whether standard or accelerated, is not appropriate for everyone. It is currently indicated for treatment-resistant major depressive disorder, meaning patients who have not responded adequately to antidepressant medication. It is not a first-line treatment, and it works best as part of a comprehensive treatment plan that may include therapy, medication, lifestyle modifications, and ongoing psychiatric care. People with certain medical conditions, including implanted metallic devices in the head, a history of seizures, or certain neurological conditions, may not be candidates for TMS. The decision to pursue brain stimulation treatment should always be made in consultation with a qualified psychiatrist who can evaluate individual risk factors and treatment history.
The broader trajectory, however, is encouraging. Between the UCLA 5x5 protocol and the Stanford SAINT protocol, the evidence is converging on a core insight: the depressed brain can absorb and benefit from intensive stimulation delivered in days rather than weeks. The remaining questions are about optimization, specifically which intensity, targeting method, and session count produces the best outcomes with the fewest side effects for the widest range of patients. Those questions will take years of research to answer fully, but for the millions of people living with treatment-resistant depression, the direction of the evidence offers genuine reason for cautious optimism.
Where to Start
If you or someone you know is living with depression that hasn’t responded to medication, TMS is worth discussing with a psychiatrist or primary care physician. The treatment has strong evidence behind it, growing insurance coverage, and an expanding network of clinics across the country. The accelerated protocols described here are still in the research phase and not yet widely available outside of academic medical centers, but the standard six-week protocol is FDA-cleared, covered by most major insurers, and accessible at hundreds of clinics nationwide.
Start by asking your physician for a referral to a TMS provider. Most clinics offer a free initial consultation to determine whether you’re a candidate based on your diagnosis and treatment history. If the six-week schedule is a barrier, ask about the availability of accelerated or compressed protocols, as more clinics are beginning to offer them in response to emerging research. The National Alliance on Mental Illness (NAMI) helpline at 1-800-950-NAMI (6264) can also help connect you with local resources and support.
Depression is a medical condition with medical treatments. No one should have to live with persistent depressive symptoms because the logistics of getting to a clinic five days a week for six weeks are unworkable. The research from UCLA and Stanford suggests that a shorter path to relief may be within reach, and that is a development worth watching closely.
Sources
- New brain stimulation approach could treat depression in just 5 days - ScienceDaily
- A depression treatment that once took eight weeks may work just as well in one - UCLA Health
- A depression treatment that once took eight weeks may work just as well in one - Medical Xpress
- Stanford Accelerated Intelligent Neuromodulation Therapy (SAINT) - Stanford Health Care
- TMS Therapy Cost Guide 2026 - Southern Live Oak Wellness