Every January, millions of people declare their dietary allegiance. Some swear by the Mediterranean approach, embracing olive oil, fish, and abundant vegetables. Others go keto, cutting carbs to near-zero and watching their bodies shift to fat-burning mode. Both camps cite research. Both report transformative results. So which diet actually produces better long-term health outcomes?
The answer, backed by a growing body of head-to-head trials, is more nuanced than either camp’s evangelists suggest. A 2-year randomized controlled trial published in the Annals of Internal Medicine (2020) directly compared Mediterranean and ketogenic diets in 322 participants with obesity and metabolic syndrome. Both groups lost weight. Both improved metabolic markers. But the patterns differed in ways that matter for different goals and different people.
The Mediterranean diet has 50+ years of research behind it, including the landmark PREDIMED trial (7,447 participants, published in NEJM) showing a 30% reduction in major cardiovascular events. The ketogenic diet has compelling shorter-term data, particularly for weight loss and glucose control, but limited evidence beyond 2 years. Understanding these trade-offs helps you make an informed choice rather than following the latest trend.
Fundamentally Different Philosophies
These two dietary patterns represent opposing nutritional philosophies, and understanding this conceptual difference helps explain why they produce different outcomes and suit different people.
The Mediterranean diet is a model of abundance and variety. It doesn’t focus primarily on restriction but rather on what to add: more olive oil, more fish, more vegetables, more legumes, more whole grains. The traditional eating patterns of Greece, Southern Italy, and Spain form its foundation. Macronutrient distribution typically falls around 40-50% carbohydrates, 30-35% fat (primarily monounsaturated from olive oil), and 15-20% protein. Red wine in moderation is permitted. Red meat is limited but not forbidden. Nothing is completely off-limits.

The ketogenic diet is a model of metabolic restriction. Its power comes from what you eliminate. By cutting carbohydrates to under 50 grams daily (often under 20 grams for therapeutic ketosis), you force a fundamental shift in fuel metabolism. Without dietary glucose, the liver begins producing ketone bodies from fat, and these ketones become the primary fuel for brain and muscle. Macronutrient distribution runs approximately 70-80% fat, 15-20% protein, and 5-10% carbohydrates. This requires eliminating bread, pasta, rice, most fruits, legumes, and many vegetables. It’s not just low-carb; it’s carb-elimination.
This philosophical divergence explains why adherence rates differ so dramatically between the two approaches. The Mediterranean diet can be adopted gradually and fits within most social eating situations. The ketogenic diet requires precision and constant vigilance, as even moderate carb intake can knock you out of ketosis and restart adaptation. One is a lifestyle that accommodates normal life; the other is an intervention that demands significant lifestyle restructuring.
Weight Loss Trajectories: Different Paths to Similar Endpoints
The 2-year head-to-head data reveals fascinating differences in how weight changes over time on each diet, with implications for both short-term motivation and long-term success.
Ketogenic dieters experienced rapid initial weight loss, averaging 12% of body weight lost by the 6-month mark, a substantial result that kept motivation high. This rapid loss includes both fat and the glycogen plus water that depletes when carbohydrate stores are exhausted. However, the trajectory shifted over time. By 12 months, average weight loss had moderated to 9% of baseline, and by 24 months, participants maintained only 7% loss from their starting weight. This pattern of faster initial loss followed by gradual regain is characteristic of restrictive diets.
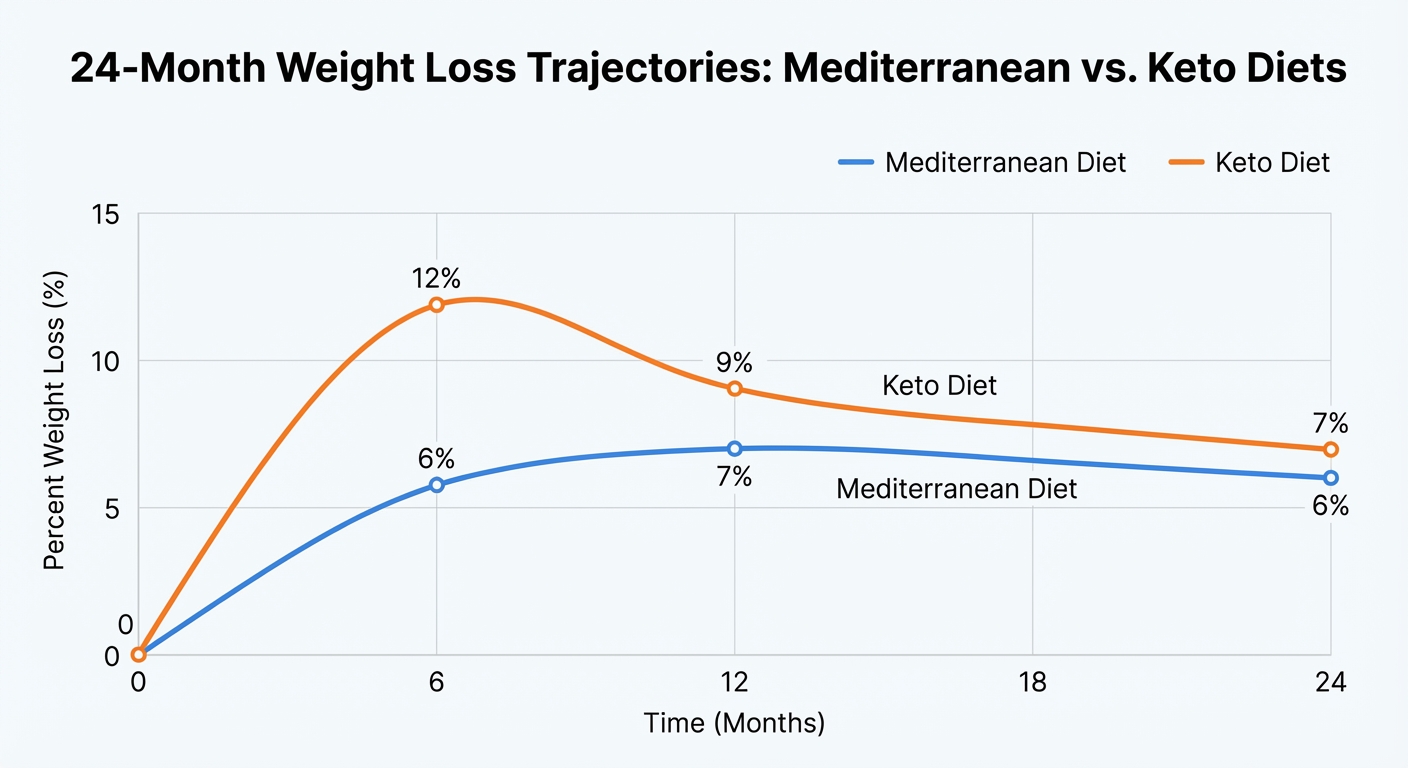
Mediterranean dieters showed a different pattern. Initial weight loss was more modest at approximately 6% of body weight at the 6-month mark, half what the keto group achieved. This slower start could feel frustrating for participants seeking rapid results. But the Mediterranean group maintained their losses better over time: 7% at 12 months and 6% at 24 months. The steadier pattern without significant rebound meant that by the 2-year endpoint, total weight loss was remarkably similar between groups, approximately 6-7% of initial body weight.
The dropout rates tell an equally important story. The keto group experienced 40% attrition by 24 months, meaning nearly half of participants couldn’t or wouldn’t continue. The Mediterranean group had only 25% dropout. When a diet is too restrictive to follow, even impressive short-term results become irrelevant. The best diet is one you can actually maintain, and the data strongly suggests Mediterranean eating is more sustainable for most people.
The interpretation depends on your priorities. If rapid initial weight loss matters for an upcoming event, medical procedure, or psychological motivation, keto delivers faster visible results. If sustainable, long-term weight management is the goal, Mediterranean’s steadier trajectory with better maintenance may be more appealing. By two years, both approaches produce similar total weight loss, but the paths differ significantly.
Cardiovascular Health: Where Mediterranean Dominates
For heart health specifically, the Mediterranean diet has vastly more supporting evidence and a proven track record of reducing the diseases that kill the most people. The comparison isn’t even close.
Lipid profiles respond differently to each diet, with important implications for cardiovascular risk. Mediterranean eating consistently reduces LDL cholesterol (“bad” cholesterol) by 10-15%, raises HDL cholesterol (“good” cholesterol) by 5-8%, and lowers triglycerides by 15-20%. This combination represents an ideal cardiovascular risk profile and explains much of the Mediterranean diet’s protective effect against heart disease.
The ketogenic diet shows more variable and potentially concerning lipid responses. Triglycerides typically decrease substantially (often 20-30%), and HDL tends to rise modestly, both favorable changes. However, LDL response is highly variable and sometimes alarming. Some individuals see minimal LDL change or even slight improvement. Others experience dramatic LDL increases of 50-100+ mg/dL, a phenomenon sometimes called “lean mass hyper-responder” pattern. For individuals whose LDL skyrockets on keto, the cardiovascular implications are uncertain but potentially concerning.
Blood pressure responds more favorably to Mediterranean eating, with systolic pressure dropping an average of 5-8 mmHg, a clinically meaningful reduction equivalent to some medications. The mechanisms include high potassium from abundant vegetables, nitric oxide production from olive oil polyphenols, and reduced sodium from minimizing processed foods. The anti-inflammatory benefits of Mediterranean eating extend beyond cardiovascular markers. Ketogenic diets show minimal blood pressure effect in most studies, with some individuals experiencing slight increases, possibly related to changes in sodium and fluid balance.
Inflammation markers, particularly C-reactive protein (CRP), decrease dramatically on Mediterranean diet. Reductions of 30-40% are typical in intervention trials, indicating substantial anti-inflammatory effects. The olive oil, fatty fish, nuts, and colorful vegetables all contribute anti-inflammatory compounds. Ketogenic diets show inconsistent inflammation responses across studies, with some showing modest reductions and others showing no change.
The most critical distinction is in proven long-term cardiovascular outcomes. The PREDIMED trial, published in New England Journal of Medicine, demonstrated a 30% reduction in major cardiovascular events (heart attacks, strokes, cardiovascular death) in the Mediterranean diet group compared to control. This wasn’t surrogate markers like cholesterol; this was actual heart attacks prevented, strokes avoided, lives extended. No ketogenic diet study has demonstrated comparable long-term cardiovascular outcome data. We simply don’t know what eating 70-80% fat for 20-30 years does to cardiovascular health.
Metabolic Health and Diabetes
Both diets improve metabolic health markers, but through fundamentally different mechanisms and with different evidence bases supporting their effects. For people with prediabetes or type 2 diabetes, both options have merit.
Glucose control improves on both diets, though through distinct pathways. The ketogenic diet produces faster absolute glucose reduction by eliminating the carbohydrates that raise blood sugar in the first place. Within days to weeks, fasting glucose drops, post-meal glucose spikes disappear, and HbA1c begins declining. For people with type 2 diabetes, this can be genuinely transformative, with some achieving complete remission (normal blood glucose without medication) through strict carbohydrate restriction.
A 2019 study published in Diabetes Therapy followed 262 patients with type 2 diabetes on a medically supervised ketogenic diet for 2 years. At the 1-year mark, 60% had reduced their HbA1c below the diabetes threshold (6.5%), and medication use (including insulin) decreased substantially. These are remarkable results that demonstrate keto’s therapeutic potential for diabetes management.

The Mediterranean diet shows more gradual but sustained glucose improvements that appear to reflect genuine improvements in underlying metabolic health rather than just carbohydrate avoidance. Insulin sensitivity improves, meaning cells become more responsive to insulin’s signals. Understanding your personal glucose response through continuous glucose monitoring can help optimize either approach. The PREDIMED trial showed a 52% reduction in new diabetes diagnoses among high-risk participants following Mediterranean diet versus control. For diabetes prevention, Mediterranean has the strongest evidence base.
For people already diagnosed with type 2 diabetes, the choice depends on goals and circumstances. Keto offers the potential for more dramatic short-term improvement and possibly remission but requires strict adherence and ongoing carbohydrate restriction. Mediterranean offers reliable, sustainable improvement that’s easier to maintain long-term. For insulin-dependent type 2 diabetics, any significant dietary change requires close medical supervision to adjust medications and prevent hypoglycemia.
Sustainability and Real-World Adherence
The best diet is the one you can actually follow. On this criterion, Mediterranean eating has significant advantages over ketogenic restriction for most people.
Adherence rates from clinical trials quantify what anyone who’s tried both diets intuitively knows. Mediterranean diets show 65-70% adherence at 2 years; ketogenic diets show only 35-45%. The dropout rate from keto is nearly double that of Mediterranean. This isn’t moral failing; it’s the predictable result of trying to maintain an extreme dietary pattern in a carbohydrate-rich food environment.
Why Mediterranean is more sustainable:
- Less restrictive, focusing on what to add rather than eliminate
- Socially compatible with restaurants, family meals, and travel
- Varied and flavorful, with cuisine from multiple cultures
- No major food groups completely forbidden
- Cultural heritage for many people, feeling like “real food” rather than a “diet”
Why keto is harder to maintain:
- Extremely restrictive (no bread, pasta, rice, most fruits, many vegetables)
- Socially challenging (most restaurants and gatherings center on carb-heavy foods)
- Requires vigilance (even moderate carb intake disrupts ketosis)
- Initial adaptation period with fatigue and “keto flu”
- Many people genuinely miss carbohydrate-rich foods
The psychological burden of extreme restriction often leads to cycles of strict adherence followed by abandonment and regain. Mediterranean’s moderate approach may produce slower initial results but avoids this boom-bust pattern. For lifetime weight management, sustainability trumps short-term dramatic results.
Who Should Consider Each Diet
Neither diet is universally optimal. Individual factors including health conditions, goals, food preferences, and lifestyle determine which approach makes more sense.
Consider Mediterranean diet if:
- Cardiovascular health is a primary concern (strongest evidence)
- You want a sustainable, long-term eating pattern
- You enjoy variety and don’t want to eliminate major food groups
- Social eating and restaurants are important to your lifestyle
- You have a history of yo-yo dieting from restrictive approaches
- You’re focused on prevention and longevity rather than therapeutic intervention
Consider ketogenic diet if:
- You have type 2 diabetes and want to attempt remission (with medical supervision)
- You have drug-resistant epilepsy (keto has strongest evidence for seizure control)
- You need rapid initial weight loss for medical reasons (pre-surgery, etc.)
- You’ve tried moderate approaches without success and want to try something different
- You respond well to structured, rule-based eating
- You don’t find carbohydrate restriction psychologically difficult
Keto is generally inappropriate for:
- Athletes requiring explosive power and glycolytic performance
- Pregnant or nursing women
- People with kidney disease
- Those with history of disordered eating
- Anyone unable to maintain close medical monitoring if taking diabetes medications
The Bottom Line
The Mediterranean diet has the strongest evidence for long-term health, cardiovascular protection, and sustainability. Five decades of research, including large randomized trials with hard cardiovascular endpoints, support its benefits. It’s the closest thing to a default recommendation that nutrition science can offer.
The ketogenic diet has strong evidence for specific therapeutic applications, including epilepsy management, rapid weight loss, and type 2 diabetes control. For these targeted uses, it can be genuinely transformative. But limited long-term safety data and poor sustainability make it a harder recommendation for general population health.
For most people seeking long-term health: Mediterranean eating is the safer, more evidence-based, more sustainable choice. Start by adding olive oil, fish, vegetables, and legumes rather than focusing on restriction.
For specific therapeutic goals: Ketogenic intervention might be appropriate, but ideally with medical supervision, clear endpoints, and a plan for transition to sustainable eating afterward.
The pragmatic approach: Most people do best with Mediterranean-inspired eating, lots of plants, healthy fats, quality proteins, minimal processed foods, without religious adherence to any specific macronutrient ratio. Eat real food. Mostly plants. Not too much. That advice remains the best-supported guidance for a healthy, sustainable relationship with food.
Sources: PREDIMED trial (NEJM 2013, 2018 correction), Annals of Internal Medicine diet comparison trials, Diabetes Therapy ketogenic diabetes studies, JAMA cardiovascular outcomes research, systematic reviews of Mediterranean and ketogenic diet evidence.