Walk into a CrossFit gym or a tech startup in 2025, and you’ll likely spot a small white disc adhered to the back of someone’s tricep. The continuous glucose monitor, once a medical device strictly for Type 1 diabetics managing insulin dosing, has gone mainstream. Companies like Levels, Nutrisense, and Signos have gamified metabolism, promising that flattening your glucose curve is the key to weight loss, sustained energy, longevity, and peak cognitive performance. The devices sell for $200-400 per month, creating a subscription market projected to reach $1.2 billion by 2027 for non-diabetic users alone.
The appeal is intuitive: real-time data about what’s happening inside your body, delivered to your phone in colorful graphs. You eat an apple and watch the line rise. You take a walk and watch it fall. The immediate feedback creates a powerful sense of control in an area of health that previously felt like a black box. Yet as CGMs have proliferated among the metabolically healthy “worried well,” a growing body of research and clinical opinion questions whether this data stream helps or harms. The answer, as with most things in nutrition, depends entirely on context.
Dr. Robert Lustig, a pediatric endocrinologist at UCSF who has spent decades researching metabolic disease, has been cautiously supportive of CGMs for education while warning against their misuse. “A CGM can be a powerful teaching tool,” he notes. “The problem is when people start treating every spike as a crisis. Glucose variability is normal. It’s how your body works.” Understanding when CGM data provides actionable insights versus when it creates unnecessary anxiety requires examining what these devices actually measure and what that data means.
What CGMs Measure and What They Don’t
A continuous glucose monitor samples interstitial fluid, the liquid surrounding cells in subcutaneous tissue, every one to five minutes depending on the device. This measurement is then algorithmically converted to an estimated blood glucose reading. The distinction matters: interstitial glucose lags behind blood glucose by approximately 5-15 minutes, which explains why CGM readings during rapid changes (immediately post-meal or during exercise) can differ substantially from a finger-stick blood test.
For diabetics managing insulin dosing, this lag is well-understood and calibration adjustments are built into clinical practice. For non-diabetics using CGMs to “optimize” their response to specific foods, the lag introduces complexity. That spike you see 45 minutes after eating might actually represent glucose levels from 30-35 minutes post-meal. The peak you’re trying to avoid may have already passed by the time you see it on screen.
Accuracy also varies between devices and between individuals. A 2021 study in Diabetes Technology & Therapeutics found that popular consumer CGMs had mean absolute relative differences (MARD) of 9-14% compared to laboratory blood glucose measurements. For clinical diabetes management, this accuracy is generally acceptable. For someone trying to determine whether oatmeal or eggs produce a “better” glucose response, the margin of error may exceed the difference being measured.
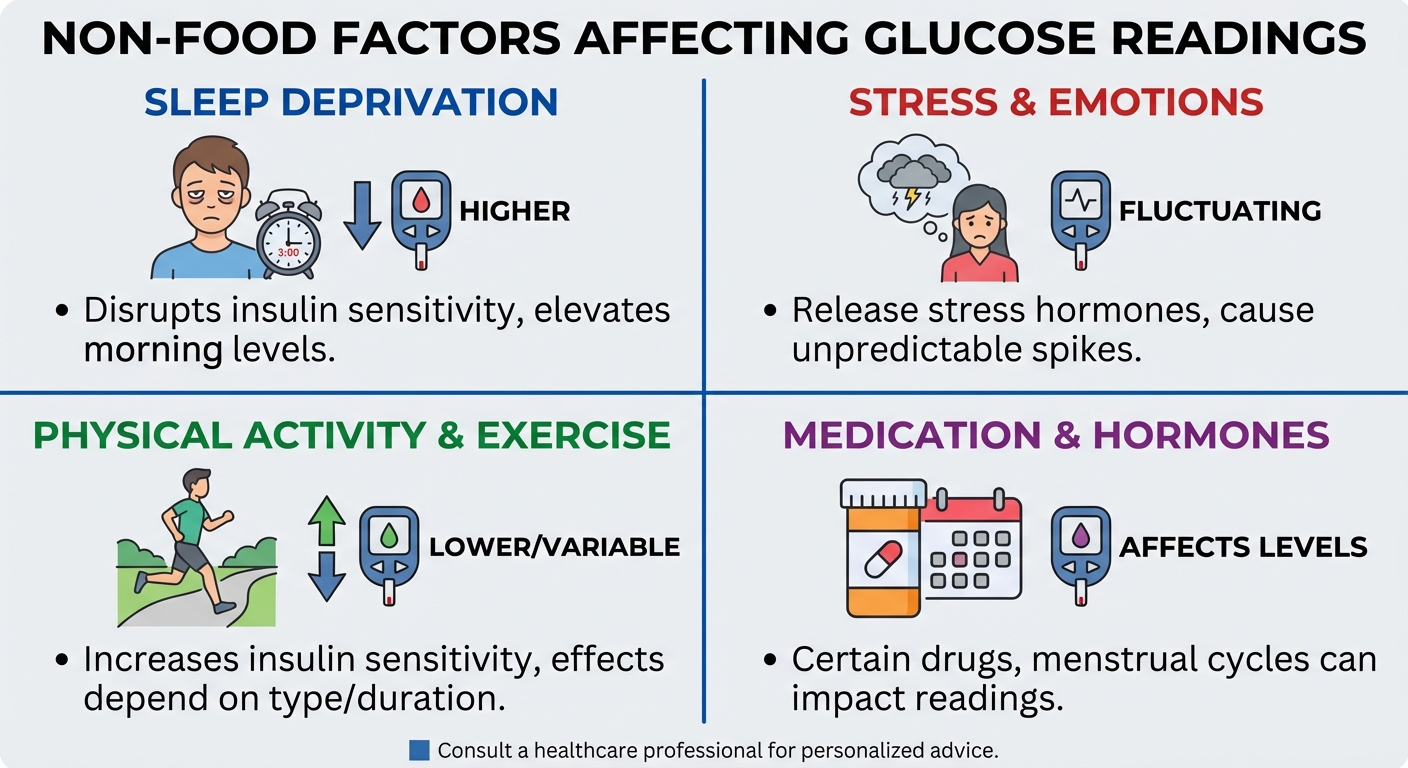
The data CGMs provide is genuinely fascinating. Users discover how non-food factors dramatically influence glucose: a poor night’s sleep can raise fasting glucose by 10-20 mg/dL, acute stress triggers cortisol-mediated glucose release, and intense exercise causes massive spikes as the liver dumps glycogen for fuel. The “Dawn Phenomenon,” where glucose rises before waking due to natural cortisol rhythms, surprises many first-time users who assume any morning elevation indicates metabolic dysfunction. Understanding these patterns can be educational, but the education comes quickly, often within the first two weeks of wear.
The Case For: Metabolic Flexibility Testing and Behavioral Feedback
The most compelling use case for CGMs in non-diabetic populations is assessing metabolic flexibility: your body’s ability to efficiently process glucose and return to baseline after meals. A truly metabolically healthy person consuming a mixed meal should see glucose rise moderately (typically peaking at 120-140 mg/dL for non-diabetics) and return to baseline (under 100 mg/dL) within approximately two hours.
If glucose remains elevated for three or more hours post-meal, or if it spikes above 160 mg/dL from moderate carbohydrate intake, this pattern may indicate early insulin resistance that standard fasting glucose tests miss. A 2019 study in Cell Metabolism by Stanford researchers found that CGM data identified “glucose dysregulation” in 25% of participants who had normal fasting glucose and HbA1c levels. These individuals showed prolonged post-meal elevations that traditional diagnostics wouldn’t capture.
For someone with a family history of Type 2 diabetes or signs of metabolic syndrome (elevated waist circumference, borderline blood pressure, or triglycerides), a two-week CGM trial can provide genuinely actionable data. If the data reveals impaired glucose disposal, interventions like increasing muscle mass (which improves glucose uptake independent of insulin), walking after meals (which significantly reduces glucose spikes), or adjusting meal composition can be implemented and their effects directly observed.
The behavioral feedback loop represents another legitimate benefit. Seeing glucose plummet because you took a 15-minute walk after dinner creates immediate positive reinforcement that abstract knowledge about exercise benefits cannot match. Users learn through direct observation that food order matters: eating protein and vegetables before carbohydrates blunts the glucose response compared to eating carbohydrates first. They discover that their “healthy” oat milk contains enough added sugar to create substantial spikes, or that the protein bar they assumed was metabolically neutral actually hits harder than expected.
This learning has value, but it’s also finite. After two to four weeks of attentive use, most patterns become apparent. You know which foods spike you, which habits help, and what your typical daily glucose range looks like. The question becomes whether continued monitoring provides additional benefit or simply generates data without new insights.
The Case Against: The Flatline Fallacy and Glucose Anxiety
The marketing message from CGM companies often implies, or states outright, that a flat glucose line represents the ideal. Levels Health originally promoted a “metabolic fitness” score that penalized glucose variability, encouraging users to avoid any food that caused visible rises. This framing fundamentally misrepresents normal physiology.
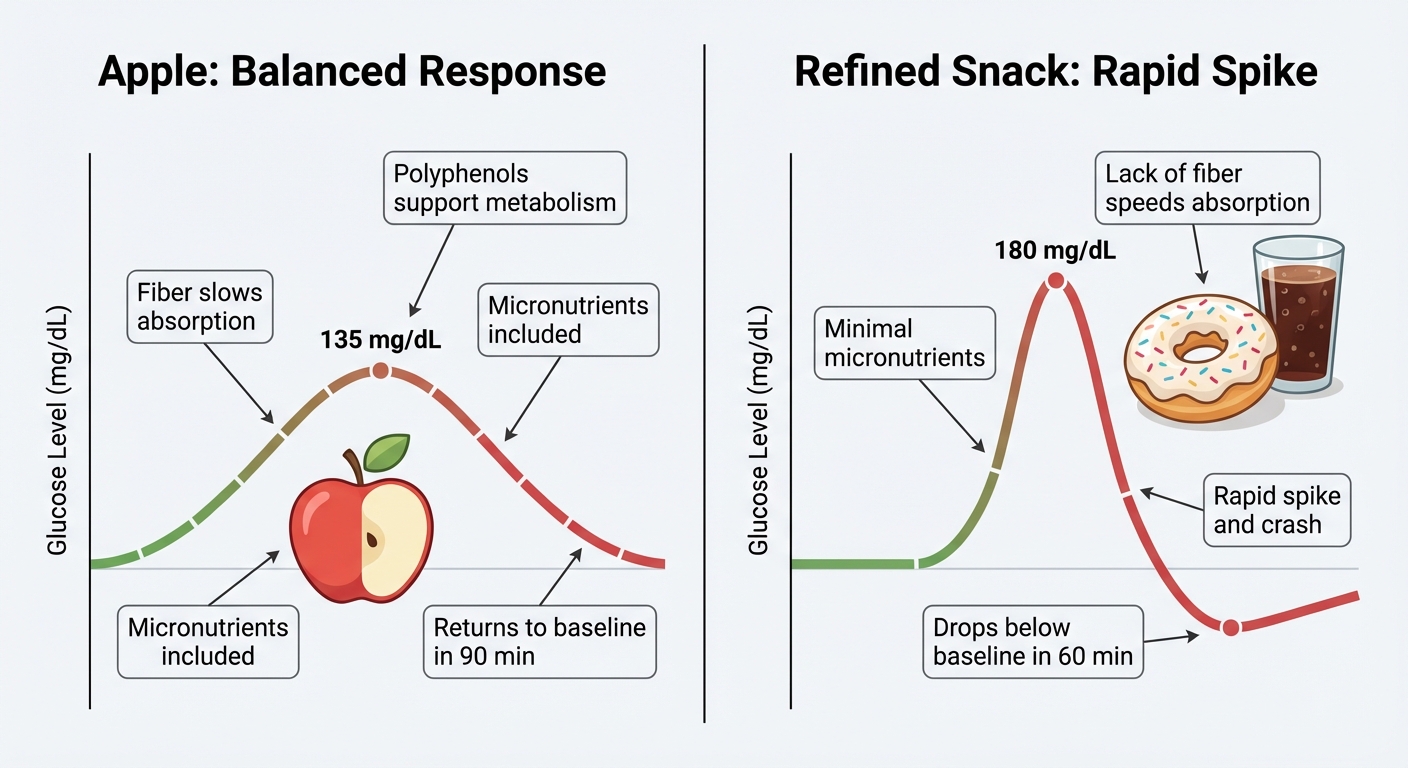
Glucose is supposed to rise after eating. The magnitude and duration of the rise depend on multiple factors: the food’s glycemic index, the presence of fiber, fat, and protein that slow absorption, your individual genetics, your gut microbiome composition, and your current metabolic state. A temporary rise to 130 mg/dL from a piece of fruit, followed by a return to baseline within 90 minutes, represents your metabolism working exactly as designed. Treating this as a problem to be eliminated creates a dysfunctional relationship with food.
Dr. Yoni Freedhoff, an obesity medicine physician at the University of Ottawa, has been vocal about CGM misuse among his non-diabetic patients. “I’ve seen people develop genuine fear of bananas because they saw a spike,” he notes. “Meanwhile, they’re eating highly processed keto bars because those keep the line flat. We’ve replaced one form of orthorexia with another.” The composition of what caused the glucose rise matters enormously. A 140 mg/dL spike from an apple with its fiber, polyphenols, and micronutrients is metabolically distinct from the same spike from a soda, even if the CGM trace looks identical.
The anxiety trap extends beyond individual food choices. Some users report checking their glucose readings 50+ times daily, experiencing genuine distress when numbers exceed arbitrary thresholds they’ve set for themselves. The gamification that makes CGMs engaging can become compulsive. A device intended to provide insight instead becomes a source of chronic stress, and stress itself raises glucose through cortisol-mediated mechanisms, creating a feedback loop of anxiety driving the very readings that cause anxiety.
Exercise-Induced Spikes: A Feature, Not a Bug
Perhaps the most commonly misunderstood CGM pattern involves exercise. High-intensity training, particularly strength training and HIIT, causes substantial glucose spikes that can alarm uninformed users. During intense exercise, the liver releases stored glycogen to provide fuel for working muscles. This hepatic glucose output can push CGM readings to 160-180 mg/dL or higher, even in highly insulin-sensitive athletes.
This response is completely normal and desirable. It represents your body mobilizing energy stores efficiently. Attempting to avoid exercise-induced glucose spikes by limiting workout intensity would be counterproductive for metabolic health. The long-term adaptations from exercise, including improved insulin sensitivity, increased muscle glucose uptake capacity, and enhanced mitochondrial function, far outweigh any concern about temporary post-workout readings.
The high-intensity interval training protocols that produce the largest glucose spikes during execution also produce the greatest improvements in metabolic flexibility over time. A 2022 study in Diabetologia found that HIIT improved insulin sensitivity more effectively than moderate continuous training despite causing higher acute glucose variability. Users who restrict exercise to avoid “bad” CGM readings are optimizing for the wrong metric.
Similarly, the glucose dip that sometimes follows intense exercise, as muscles actively uptake glucose from the bloodstream, can trigger unnecessary alarm. Seeing glucose drop to 65-70 mg/dL after a hard workout, which typically resolves within an hour, doesn’t indicate hypoglycemia requiring intervention in a non-diabetic. It indicates that your muscles are efficiently clearing glucose from circulation.
Who Actually Benefits: A Framework for Decision-Making
Based on current evidence and clinical practice patterns, CGM use provides meaningful value for specific populations while offering diminishing returns for others.
Strong candidates for CGM use include individuals with prediabetes (HbA1c 5.7-6.4% or fasting glucose 100-125 mg/dL), those with family history of Type 2 diabetes seeking early detection of glucose dysregulation, people who have struggled with weight and want to understand their individual food responses, and anyone who finds data-driven feedback genuinely motivating rather than anxiety-provoking. For these groups, even a two to four week trial can provide actionable insights that inform long-term behavior change.
Populations with diminishing CGM returns include lean, metabolically healthy individuals with normal glucose markers (HbA1c under 5.4%, fasting glucose under 95 mg/dL), those with history of disordered eating or obsessive tendencies around health metrics, endurance athletes whose training creates glucose patterns that don’t respond to dietary optimization, and anyone finding that CGM data increases rather than decreases food-related anxiety.
A reasonable middle path for the curious but healthy: wear a CGM for 14 days once per year to check baseline metabolic function and learn your personal glucose responses to common foods. This provides the educational benefit without the costs (financial and psychological) of continuous monitoring. If the two-week trial reveals normal glucose handling, there’s minimal benefit to continued wear. If it reveals concerning patterns, those patterns warrant medical follow-up regardless of continued CGM use.
The Bottom Line
Continuous glucose monitors provide a genuinely novel window into metabolic function that was previously unavailable outside clinical settings. The data is real, and for people with glucose dysregulation, it can drive meaningful behavior change. However, the consumer CGM market has grown faster than the evidence supporting its use in metabolically healthy populations, creating a category of “worried well” users who may be harming rather than helping their relationship with food.
Glucose is supposed to fluctuate. It rises after eating, falls during fasting, spikes during exercise, and responds to sleep, stress, and circadian rhythms. Treating every rise as a problem to be eliminated fundamentally misunderstands normal physiology and can drive restrictive eating patterns that prioritize glycemic flatness over nutritional adequacy. A diet that keeps glucose perfectly stable but eliminates fruit, whole grains, and legumes has not improved health outcomes.
For those who do use CGMs, the key is treating the data as information rather than judgment. Learn your patterns, understand your responses, and then apply that knowledge without the device. The goal is metabolic insight that informs better choices, not metabolic surveillance that generates chronic anxiety. If the data stream is causing more stress than the food choices it’s meant to optimize, the device has become counterproductive.
When to Consider a CGM:
- HbA1c between 5.7-6.4% (prediabetes range)
- Family history of Type 2 diabetes and desire for early detection
- Unexplained energy crashes or weight loss resistance despite dietary intervention
- Genuine curiosity combined with psychological resilience around health data
When to Skip or Discontinue:
- Normal metabolic markers and no risk factors
- Finding yourself anxious about food choices the CGM reveals
- Avoiding nutritious foods solely because of glucose response
- Checking readings compulsively throughout the day
Sources: Cell Metabolism Stanford glucose variability study (2019), Diabetes Technology & Therapeutics CGM accuracy analysis (2021), Diabetologia HIIT and insulin sensitivity research (2022), American Diabetes Association CGM position statement, Dr. Robert Lustig metabolic health research (UCSF), Dr. Yoni Freedhoff clinical observations (University of Ottawa).