Every cell in your body keeps time. From the liver cells processing nutrients on schedule to the immune cells ramping activity at specific hours, a master clock in your brain coordinates this symphony of biological rhythms. This circadian system, evolved over millions of years in sync with the rising and setting sun, expects light as its primary synchronizing signal. Morning brightness says “wake up”; evening darkness says “wind down.” When these signals match the solar pattern, the system runs smoothly. When they don’t, nearly every aspect of health suffers.
Modern life delivers exactly the wrong light pattern. We spend most of our waking hours indoors under artificial lighting that registers as dim twilight to our photoreceptors, perhaps 200-500 lux compared to the 10,000-100,000 lux of outdoor daylight. Then we stare at bright screens emitting blue-rich light in the evening, precisely when our circadian system expects darkness. The result is a population with chronically misaligned circadian rhythms, contributing to an epidemic of insomnia, depression, anxiety, and metabolic dysfunction.
Light therapy, the deliberate use of bright light exposure at specific times, offers a direct intervention for circadian misalignment. This isn’t a wellness trend or pseudoscience; it’s applied chronobiology backed by decades of clinical research. For seasonal affective disorder, light therapy is the first-line treatment recommended by the American Psychiatric Association. For non-seasonal depression, sleep disorders, and general mood optimization, the evidence base continues to grow. Understanding how light affects your brain opens practical avenues for improving mood, energy, and sleep.
The Neuroscience of Light and Mood
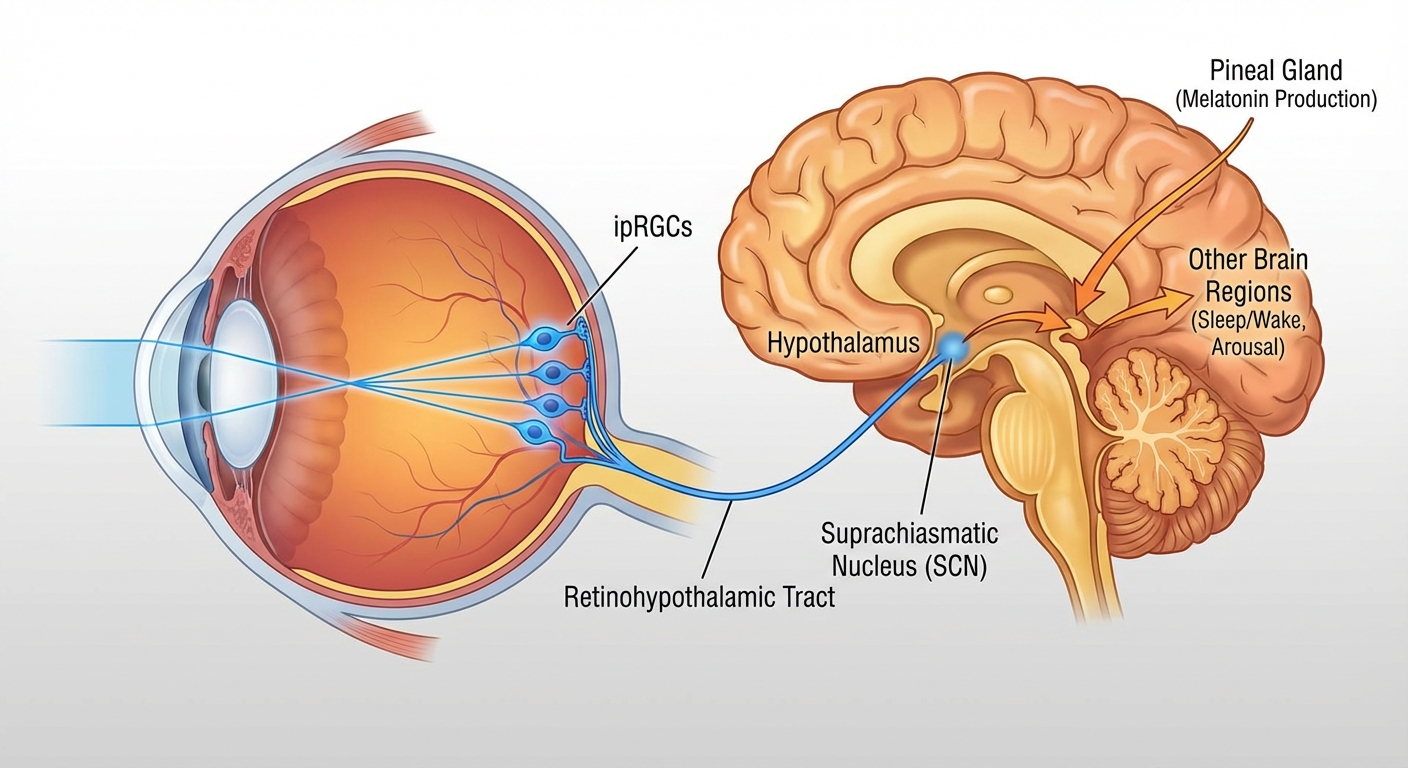
Light enters your eyes and hits specialized photoreceptor cells called intrinsically photosensitive retinal ganglion cells (ipRGCs). These cells contain melanopsin, a light-sensitive protein tuned specifically to blue-wavelength light around 480 nanometers. Critically, ipRGCs don’t contribute to vision; you could have no functional rods or cones for visual perception and still receive circadian light signals through these cells. Their sole purpose is detecting light levels and transmitting that information to the suprachiasmatic nucleus (SCN), the master clock in your hypothalamus.
The SCN receives this light input and coordinates a cascade of responses throughout the brain and body. Morning bright light triggers cortisol release from the adrenal glands, the hormone that promotes wakefulness and alertness when released on a healthy schedule. It simultaneously suppresses melatonin, the sleep hormone that should be undetectable during daytime hours. It advances circadian phase, meaning it makes you naturally alert earlier in the day and naturally tired earlier in the evening. Through connections with serotonin-producing neurons in the raphe nuclei, bright light enhances serotonin synthesis and release, a mechanism directly relevant to mood and the reason light therapy works for depression.
Evening darkness allows the reverse processes. As light levels drop, the pineal gland begins melatonin production, with levels rising throughout the evening to prepare the body for sleep. Cortisol levels decline. Core body temperature drops. The circadian system shifts toward restoration mode. When bright light disrupts this evening process, particularly the blue-rich light from screens, melatonin suppression delays sleep onset, reduces sleep quality, and shifts the entire circadian rhythm later, creating a cycle of insufficient sleep and misaligned rhythms.
Light Therapy for Seasonal Affective Disorder
Seasonal Affective Disorder (SAD) affects approximately 5% of Americans, with symptoms appearing in fall as daylight hours decrease and lifting in spring as they extend. Unlike the “winter blues” that many people experience as mild preference for warmth and light, clinical SAD involves genuine major depressive episodes: persistent low mood, anhedonia (inability to experience pleasure), fatigue, hypersomnia, carbohydrate cravings, and social withdrawal. The condition meets diagnostic criteria for major depression; it simply follows a seasonal pattern.
The cause relates directly to light deprivation. At higher latitudes, winter days may provide only 6-8 hours of weak daylight, much of which people miss by spending mornings and evenings indoors. The circadian system, receiving insufficient light input to maintain proper synchronization, drifts out of alignment with the social clock. Melatonin production remains elevated into morning hours; cortisol rhythms flatten; serotonin synthesis decreases. The neurobiological result resembles other forms of depression.
Light therapy addresses the root cause by providing the bright light signal the circadian system needs to function properly. Standard protocol involves 10,000 lux exposure for 20-30 minutes within the first hour after waking, continued daily throughout the fall and winter months. The timing matters: morning light advances circadian phase and suppresses lingering melatonin, both appropriate for treating the phase-delayed pattern typical in SAD. Evening light would worsen phase delay and is contraindicated.
Clinical trials consistently show 50-80% of SAD patients responding to light therapy, with effect sizes comparable to or exceeding antidepressant medications. A 2015 meta-analysis in the American Journal of Psychiatry found light therapy significantly superior to placebo for SAD, with a number needed to treat of 4, meaning one additional patient responds to light therapy for every four treated compared to placebo. Improvement typically begins within 1-2 weeks, with full effect by 4 weeks. The American Psychiatric Association recommends light therapy as first-line treatment for SAD, to be tried before or alongside medication.
Beyond Seasonal Depression
While light therapy gained its reputation treating winter depression, the underlying mechanism, circadian regulation affecting serotonin and other mood-relevant systems, suggests broader applications. Research increasingly supports light therapy for non-seasonal depression, with results that challenge the assumption that SAD is fundamentally different from other depression.
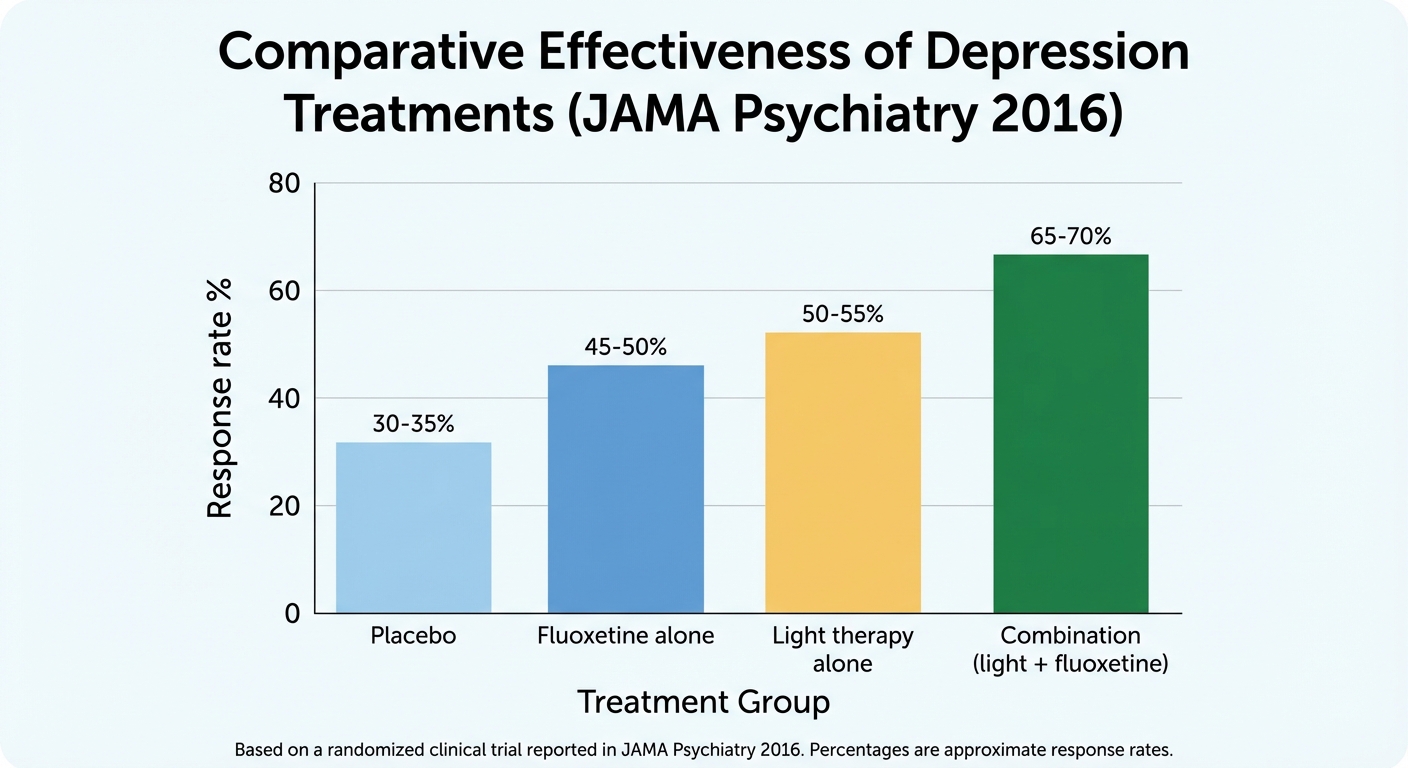
A landmark 2016 trial published in JAMA Psychiatry compared bright light therapy, fluoxetine (Prozac), their combination, and placebo in patients with non-seasonal major depression. Light therapy alone produced significantly greater improvement than fluoxetine alone, a finding that surprised many in the field. The combination of light plus fluoxetine outperformed either treatment individually. This wasn’t a small study: 122 patients over 8 weeks, randomized and placebo-controlled.
Subsequent meta-analyses find more modest but consistently positive effects for light therapy in non-seasonal depression, typically around 20-30% symptom improvement. This is meaningful as an adjunct to other treatments, particularly given the low cost, minimal side effects, and rapid onset of effect. For mild depression or depressive symptoms that don’t meet diagnostic criteria, light therapy offers an evidence-based option before or alongside pharmaceutical treatment.
The mechanism in non-seasonal depression likely relates to the circadian disruption common in depression regardless of season. Depressed patients frequently show flattened or phase-shifted cortisol rhythms, disrupted sleep architecture, and abnormal melatonin patterns. By anchoring the circadian system, bright light may restore normal neurobiological rhythms that support mood regulation. Some researchers argue that depression and circadian disruption are more interconnected than our diagnostic categories suggest.
For deeper coverage of managing seasonal affective disorder, our comprehensive guide covers light therapy alongside other evidence-based interventions.
Optimizing Sleep Through Light
Light therapy’s effects on sleep follow directly from circadian physiology. By strengthening the synchronizing signal that the circadian clock needs, properly timed light exposure improves sleep onset, sleep quality, and daytime alertness.
Morning bright light is particularly effective for people with delayed sleep phase, the night-owl pattern where natural sleep onset occurs late (1-3 AM or later) and natural wake time is correspondingly late. This common pattern, affecting perhaps 10-15% of the population to clinically significant degrees, results from a circadian clock running on a cycle slightly longer than 24 hours without sufficient morning light to advance it each day. Bright light exposure immediately upon waking (10,000 lux for 30-60 minutes) shifts the circadian phase earlier, gradually moving natural sleep onset to an earlier, more socially compatible time.
Evening light avoidance is equally important for sleep optimization. Blue-wavelength light exposure in the hours before bed suppresses melatonin production by 50% or more, directly delaying sleep onset and reducing subsequent sleep quality. The screens that dominate modern evenings, phones, tablets, computers, televisions, emit exactly the blue-rich light that maximally activates melanopsin in ipRGCs. Even “night mode” or “night shift” settings reduce but don’t eliminate this effect.
Research from Harvard and other institutions finds that bright light exposure in the two hours before bed delays the circadian clock by about an hour compared to dim light conditions. This single hour of phase delay means you want to sleep an hour later, wake an hour later, and feel groggy and unrested if forced to wake at your regular time. Repeated nightly, this creates chronic sleep deprivation and circadian misalignment even in people who believe they’re getting enough hours of rest.
The practical prescription for sleep optimization combines both elements: bright light (natural or artificial) in the first hour after waking, and dim, warm-toned light with minimal screen exposure in the 2-3 hours before bed. This creates the strong light-dark contrast the circadian system evolved to receive and now rarely gets in modern indoor environments.
Practical Light Therapy Protocols
Implementing light therapy requires appropriate equipment, positioning, timing, and duration. The details matter; a dim desk lamp or brief glance at a window won’t produce clinical effects.
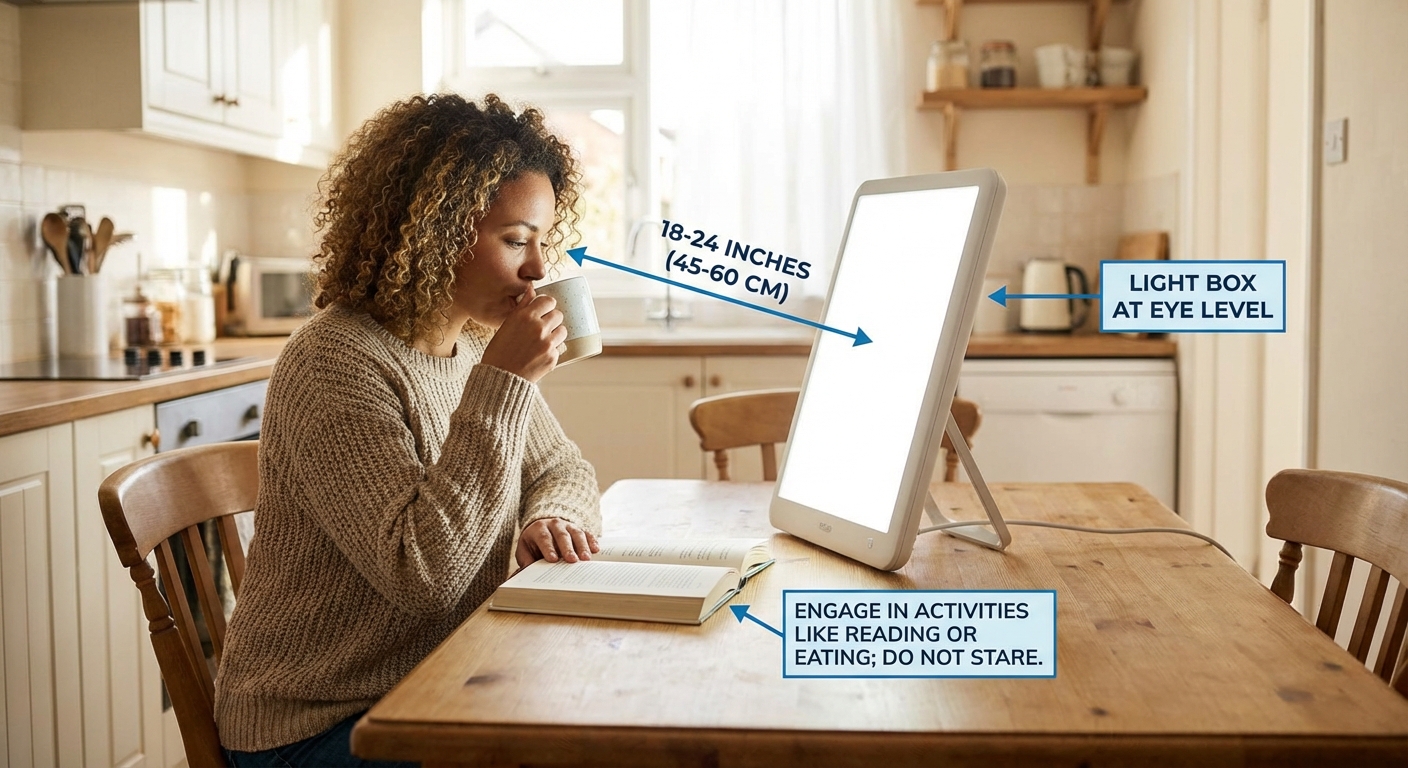
For SAD or depression treatment, use a light box delivering 10,000 lux at the recommended distance (typically 16-24 inches from your face). Many marketed “light therapy” devices don’t actually deliver 10,000 lux at usable distances; verify specifications before purchase. The light should be UV-filtered for eye safety and large enough to provide even illumination across your visual field. Small, phone-sized devices rarely deliver adequate intensity. Reputable brands with clinical research include Carex, Northern Light Technologies, Verilux, and Alaska Northern Lights, with prices ranging from $40-150.
Position the light box at eye level or slightly above, allowing light to enter your eyes indirectly. You don’t stare directly at the light; you sit in front of it while doing other activities like eating breakfast, reading, or working on a computer. The light hits your eyes from your peripheral vision. Glance at the light occasionally but don’t stare continuously.
Timing should be within the first hour after waking, ideally before 10 AM for most people. Earlier is generally better for phase-advancing effects. Using light therapy in the afternoon provides minimal circadian benefit and in the evening can worsen sleep by delaying phase.
Duration at 10,000 lux is 20-30 minutes daily for SAD treatment. Some people need longer sessions (45-60 minutes) for full effect, particularly with lower-intensity devices. You can split sessions if needed, though single continuous sessions are typical. Consistency matters more than occasional longer sessions; daily use throughout the vulnerable season produces best results.
Natural Light: The Free Alternative
Before investing in light boxes, maximize your natural light exposure. Outdoor daylight provides 10,000-100,000 lux depending on weather and time of day, far exceeding what most artificial sources deliver. Even a cloudy day provides 1,000-10,000 lux, substantially brighter than typical indoor lighting.
Morning outdoor exposure for 10-30 minutes within the first hour of waking provides free, full-spectrum light therapy. Face toward the direction of sunrise if possible. Walk, sit on a porch, drink coffee outside, or simply stand in your yard. This exposure doesn’t require direct sunlight hitting your eyes; being outdoors in daylight is sufficient. The benefits extend beyond circadian effects to include vitamin D synthesis, time in nature, and often physical activity.
For those with schedules allowing it, regular outdoor time throughout the day maintains strong circadian signaling. Working near windows, taking lunch breaks outside, and spending weekend time in natural light all contribute. The intensity difference between indoor and outdoor light is dramatic: a well-lit office provides perhaps 500 lux while the outdoor shade might provide 5,000 lux.
Natural light’s advantages include that it’s free, provides full-spectrum illumination including wavelengths not present in most artificial light sources, and often combines with other beneficial activities. Its limitations are weather-dependence and seasonal variation. In winter at high latitudes, mornings are dark, and weather may prevent outdoor time. Light boxes provide the controlled, reliable exposure that natural light can’t always guarantee.
For most people, the ideal approach combines both: maximize natural light exposure when available, and use a light box when circumstances prevent adequate outdoor time. During winter months at northern latitudes, or for shift workers whose schedules preclude normal light exposure, light boxes become essential rather than supplementary.
The Evening Light Problem
While morning light gets most attention in light therapy discussions, evening light management is equally critical for circadian health. The epidemic of sleep problems and mood disorders in modern society relates as much to excessive evening light as to insufficient morning light.
Blue-wavelength light from screens suppresses melatonin production dramatically. A 2015 study found that reading on an iPad for four hours before bed (compared to reading a physical book) reduced melatonin by 50%, delayed melatonin onset by 1.5 hours, delayed circadian phase by more than an hour, and reduced REM sleep the following night. Participants felt less sleepy at bedtime and more tired the next morning despite spending the same time in bed. This was from just four hours of typical screen use, not extreme exposure.
The solutions range from ideal to practical. Ideally, you would eliminate screens entirely for 2-3 hours before bed, using this time for reading physical books, conversation, light preparation for the next day, or relaxation activities. This is the approach most aligned with circadian biology but least compatible with modern lifestyles.
Practically, several harm-reduction strategies help. Blue-light blocking glasses with amber or orange lenses block the wavelengths that most affect melanopsin, substantially reducing melatonin suppression from screen use. Studies show amber lens glasses worn for 2 hours before bed significantly improve sleep quality and mood. Screen settings like Night Shift (iOS), Night Mode (Android), and f.lux (computers) reduce blue light emission, though less effectively than physical glasses. Switching to dim, warm-toned lighting throughout your home in the evening signals day’s end to your circadian system.
Our guide on sleep hygiene during short days provides detailed protocols for optimizing both morning light and evening darkness during winter months.
Who Benefits Most
Light therapy offers significant benefits for specific populations while providing general circadian optimization for nearly everyone.
Seasonal affective disorder patients represent the primary indicated population with the strongest evidence. If you experience reliably recurring depression during fall/winter that remits in spring/summer, light therapy should be first-line treatment, tried before or alongside medication.
Non-seasonal depression, particularly mild to moderate severity, may respond to light therapy as monotherapy or as an adjunct to medication and psychotherapy. The evidence isn’t as strong as for SAD, but the low risk and potential benefit make it reasonable to try, especially if circadian disruption (sleep problems, fatigue, diurnal mood variation) is prominent.
Sleep disorders involving circadian misalignment benefit substantially from light therapy. Delayed sleep phase disorder responds well to morning light, while advanced sleep phase (falling asleep and waking too early, more common in older adults) may respond to evening light therapy. Shift workers can use strategically timed light exposure to help shift their circadian rhythm to match their work schedule.
General population benefits include improved mood, energy, and sleep quality even in people without clinical conditions. The circadian disruption of modern indoor living affects most people to some degree. Correcting this through appropriate light exposure produces subtle but meaningful improvements in wellbeing.
The Bottom Line
Light is the most powerful signal for your circadian system, and most people in modern society get the pattern exactly wrong: too little bright light in the morning, too much blue light in the evening. This mismatch contributes to the epidemic of sleep problems, depression, and fatigue that characterizes contemporary life.
Light therapy, properly implemented, addresses this mismatch directly. For seasonal affective disorder, it’s first-line treatment with decades of research support. For non-seasonal depression and sleep disorders, it’s a low-risk adjunct with meaningful evidence. For anyone seeking to optimize mood, energy, and sleep, it’s a tool worth considering.
The essential principles are simple: get bright light exposure in the first hour after waking, whether from outdoor daylight or a 10,000 lux light box; reduce bright light exposure, especially from screens, in the 2-3 hours before bed; and maintain this pattern consistently. Your circadian system will respond to these signals by aligning more closely with the pattern it evolved to expect, and your mood, energy, and sleep will improve accordingly.
Your Light Therapy Protocol:
- Maximize morning light: get outside for 10-30 minutes within an hour of waking, or use a 10,000 lux light box for 20-30 minutes
- Maintain daytime light: work near windows when possible, take breaks outside
- Reduce evening light: dim household lighting 2 hours before bed, use warm-toned bulbs
- Limit screens before bed: avoid screens for 1-2 hours before sleep, or use blue-blocking glasses
- Create dark sleeping environment: blackout curtains, remove light-emitting devices
- For SAD: start light therapy in early fall before symptoms onset, continue through spring
Sources: JAMA Psychiatry light therapy and depression trials, American Journal of Psychiatry SAD meta-analyses, chronobiology research on melanopsin and ipRGCs, Harvard sleep and circadian research, Proceedings of the National Academy of Sciences screen light studies, American Psychiatric Association treatment guidelines.