
You’ve probably heard you need about 50 grams of protein per day. That’s the rough translation of the Recommended Dietary Allowance (RDA) for a 150-pound person, and for decades it was treated as adequate for basically everyone. Hit that number, the thinking went, and you’re covered.
Except the science has evolved substantially, and the old recommendation now looks woefully inadequate for many populations. The RDA was established through nitrogen balance studies designed to determine the minimum protein needed to prevent deficiency in sedentary adults, not the amount needed to thrive, build muscle, age well, or preserve lean mass during weight loss. It answers “how little can you eat without getting sick?” rather than “how much supports optimal health and function?”
This distinction matters more than ever as new health challenges emerge. The explosion of GLP-1 medications like Ozempic and Mounjaro for weight loss has created a protein crisis for millions of users who can barely eat enough to survive, let alone meet elevated protein needs during rapid weight loss. Growing awareness of sarcopenia, the age-related muscle wasting that begins earlier and progresses faster than most people realize, has researchers recommending dramatically higher intakes for older adults. And the sports nutrition literature has long established that active individuals need protein levels far above the RDA to support training adaptations and recovery.
Understanding your actual protein needs requires looking at your age, activity level, goals, and current health circumstances. The answer isn’t one-size-fits-all, but the direction of the science is clear: most people eating “adequate” protein by old standards are actually falling short.
Why the RDA Is a Floor, Not a Target
The RDA of 0.8 grams of protein per kilogram of body weight (roughly 0.36 grams per pound) represents the minimum intake needed to maintain nitrogen balance in most sedentary adults. Nitrogen balance means you’re replacing the protein your body breaks down each day without either losing or gaining protein stores. It’s a survival threshold, not an optimization target.
The methodology behind the RDA has been criticized by protein researchers for decades. The studies that established it examined sedentary adults under controlled laboratory conditions, not active people in real-world environments. They measured the minimum needed to prevent measurable deficiency, not the amount that supports muscle maintenance, immune function, satiety, or the many other roles protein plays beyond basic survival.
Consider the analogy to other nutrients. The RDA for vitamin C is the amount needed to prevent scurvy, not the amount that optimizes immune function. You can survive on 10mg of vitamin C daily without developing scurvy, but that doesn’t mean 10mg represents optimal intake. The same logic applies to protein: you can maintain nitrogen balance on 0.8g/kg, but that doesn’t mean you’re thriving.
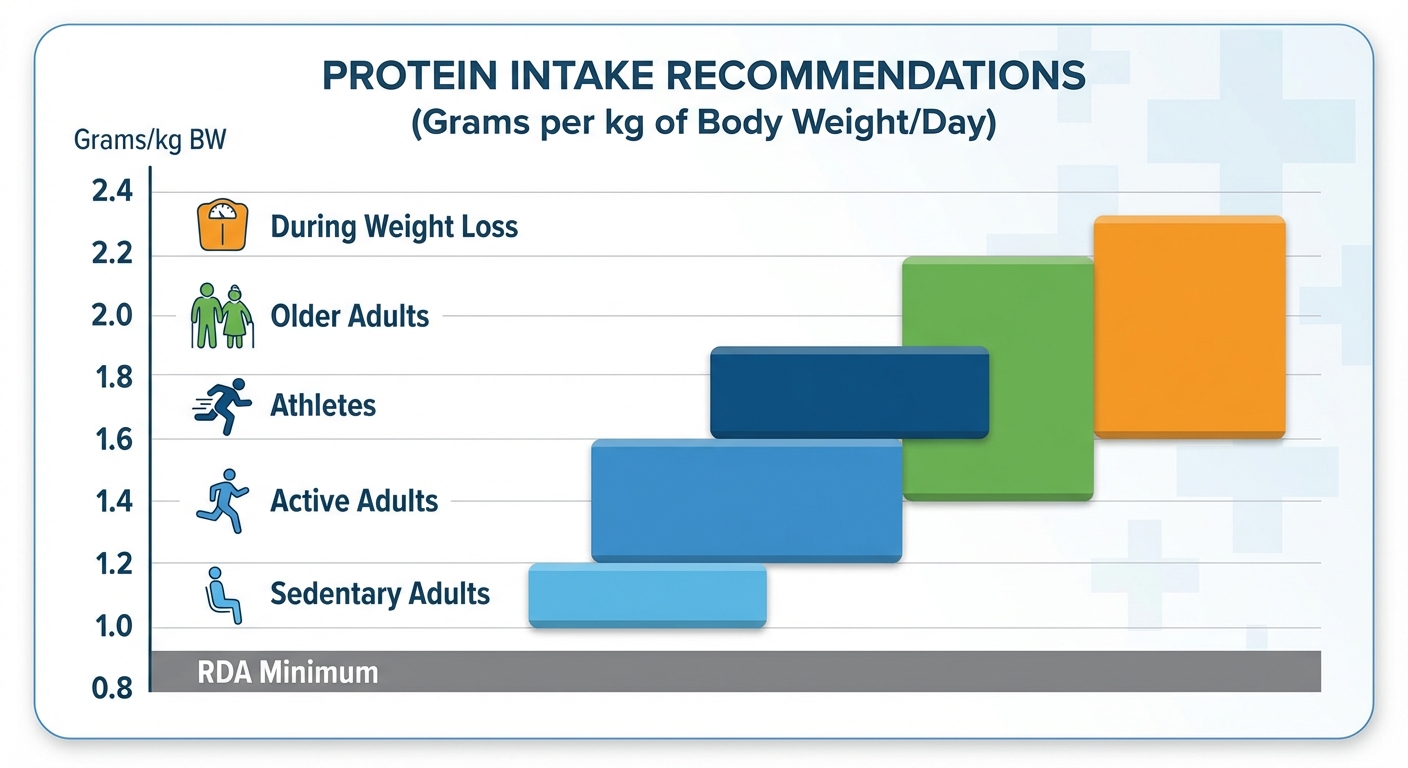
Research from the American Journal of Clinical Nutrition and the International Society of Sports Nutrition suggests that optimal protein intake for most healthy adults falls in the range of 1.2-2.2g/kg (roughly 0.55-1.0g per pound), depending on goals and circumstances. That’s 50-150% more than the RDA recommends. For a 150-pound person, this translates to roughly 80-150 grams daily rather than the RDA’s 54 grams.
Protein Needs Across the Lifespan
Your protein requirements change substantially as you age, generally increasing even as caloric needs decrease. This creates a nutritional challenge: older adults often eat less overall while needing more of each calorie to come from protein.
Young adults (18-40) have the most flexibility. Sedentary individuals in this age range can probably get by with the standard RDA, though even they would likely benefit from more. Active adults need 1.2-1.6g/kg to support exercise recovery and maintain muscle mass. Those actively trying to build muscle benefit from the higher end of this range, around 1.6-2.2g/kg, with research from the Journal of the International Society of Sports Nutrition showing that muscle protein synthesis plateaus around 1.6g/kg daily, with diminishing returns beyond 2.2g/kg for most people.
Middle-aged adults (40-65) face the beginning of anabolic resistance, a reduced efficiency in using dietary protein to build and maintain muscle. A 50-year-old’s muscles don’t respond to the same protein dose as effectively as a 25-year-old’s muscles do. Combined with the natural decline in muscle mass that accelerates after 40 (roughly 3-8% per decade without intervention), this means middle-aged adults need more protein just to maintain the same muscle mass. Research from the Journal of Nutrition Health and Aging suggests 1.2-1.6g/kg for maintenance, with higher intakes during weight loss to preserve lean mass.
Older adults (65+) have the highest requirements relative to body weight. A 2019 systematic review in Nutrients found that adults over 65 consuming 1.5-2.0g/kg showed significantly better muscle mass, strength, and functional capacity than those at lower intakes. The anabolic resistance that begins in middle age intensifies with each decade, meaning older muscles need a stronger protein signal to respond. Frailty, falls, and loss of independence are often rooted in muscle loss that adequate protein intake, combined with resistance training, can help prevent or slow.
Athletes and heavy exercisers have clearly elevated needs beyond the general population. Endurance athletes require 1.2-1.6g/kg to support recovery from training and prevent the muscle breakdown that can occur during extended exercise. Strength athletes benefit from the higher range of 1.6-2.2g/kg to maximize muscle protein synthesis. During intense training blocks or caloric restriction phases, needs may reach 2.4g/kg. The International Society of Sports Nutrition position stand recommends 1.4-2.0g/kg for most athletes as a general target.
The GLP-1 Medication Challenge
The emergence of GLP-1 receptor agonists like semaglutide (Ozempic, Wegovy) and tirzepatide (Mounjaro, Zepbound) for weight loss has created perhaps the most urgent protein adequacy crisis in modern nutrition. These medications cause dramatic appetite suppression, often reducing intake to 800-1,200 calories daily. Patients frequently report struggling to eat at all, let alone prioritize protein.
The problem is severe: studies show that 25-40% of weight lost on GLP-1 medications can be lean mass (muscle and bone) rather than fat, particularly when protein intake is inadequate and resistance training is absent. This isn’t just a cosmetic concern. Losing substantial muscle mass during weight loss tanks metabolic rate, making weight regain more likely once medication stops. It compromises functional capacity, especially in older adults. And it accelerates the trajectory toward sarcopenia and frailty.
Emerging protocols from bariatric medicine and obesity specialists emphasize that protein must be the absolute priority for anyone on these medications. Every meal and snack should be protein-forward. Recommended intakes are calculated based on goal body weight rather than current weight, typically 1.2-1.6g/kg of ideal body weight at minimum, with 1.6-2.0g/kg optimal when combined with resistance training.
Practically, this means someone with a goal weight of 150 pounds (68kg) should aim for 80-135 grams of protein daily while eating total calories that may barely exceed 1,000. That requires protein to comprise 35-50% of total calories, dramatically higher than the typical 15-20%. Protein shakes, Greek yogurt, cottage cheese, egg whites, and lean meats become staples by necessity. Without strategic protein prioritization and resistance training, people lose weight on GLP-1s but emerge weaker, with lower metabolic rates, and at higher risk of rapid regain.
Protein Quality: Not All Grams Are Equal
Total daily protein matters, but so does the quality of your protein sources. Different foods contain different amino acid profiles and are digested and absorbed with varying efficiency.
Complete proteins contain all nine essential amino acids (the ones your body cannot synthesize) in amounts adequate for human needs. Animal proteins, eggs, dairy, meat, fish, and poultry, are all complete proteins. Among plant sources, soy and quinoa are considered complete. Most other plant proteins are “incomplete,” lower in one or more essential amino acids, typically lysine in grains and methionine in legumes.
This doesn’t mean plant proteins are inferior, but it does mean vegetarians and vegans need to eat more total protein and vary their sources throughout the day to ensure adequate essential amino acid intake. Research suggests plant-based athletes should aim for protein intakes 10-20% higher than omnivore athletes to achieve equivalent muscle building effects.
Leucine content is particularly important for muscle protein synthesis. Of the nine essential amino acids, leucine is the primary trigger that signals muscles to build new protein. You need roughly 2-3 grams of leucine per meal to maximally stimulate muscle protein synthesis. Animal proteins are typically 8-10% leucine, while most plant proteins are 6-7% leucine. This means hitting the leucine threshold requires about 25-30 grams of animal protein per meal, versus 35-45 grams of plant protein.
Bioavailability measures how much of the protein you eat actually gets absorbed and used by your body. The DIAAS (Digestible Indispensable Amino Acid Score) is the current gold standard measurement. Whey protein, egg whites, chicken, and fish score highest (above 100). Beef, pork, soy, and milk score high (75-100). Chickpeas, lentils, and rice score moderate (50-75). Wheat, nuts, and most vegetables score lower (below 50). This explains why 100g of chicken supports muscle building more effectively than 100g of wheat gluten despite similar total protein content.
Optimal Protein Distribution
How you distribute protein across meals matters nearly as much as how much you eat in total. Your muscles can only use a finite amount of protein per eating occasion to stimulate muscle protein synthesis. Eating 100 grams in one sitting doesn’t provide three times the muscle-building benefit of eating 35 grams.
Research suggests that 25-40 grams of high-quality protein per meal maximizes muscle protein synthesis for most people. Eating more than this doesn’t hurt, but it doesn’t provide additional muscle-building benefits. The excess protein gets oxidized for energy or converted to other purposes. This is why spreading protein across 3-4 meals typically works better than front-loading at dinner, as many people do, or consuming most protein in a single large meal.
A practical distribution for someone targeting 120 grams daily might look like:
- Breakfast: 30g (3 eggs + Greek yogurt = ~28g)
- Lunch: 35g (6oz chicken breast = ~35g)
- Dinner: 35g (6oz salmon = ~34g)
- Snack: 20g (cottage cheese or protein shake)
This keeps muscle protein synthesis elevated throughout the day rather than spiking once and dropping.
Pre-sleep protein represents one exception to the “spread it out evenly” principle. There’s strong evidence that a protein-rich snack before bed, particularly slow-digesting protein like casein from dairy, supports overnight muscle recovery and maintenance. Studies show 30-40g of protein consumed 30 minutes before sleep can improve muscle mass and strength gains over time. Greek yogurt, cottage cheese, or a casein protein shake are common choices for this purpose.
Meeting Higher Protein Targets: Practical Strategies
Once you understand your target, the practical challenge becomes actually hitting it. Many people dramatically underestimate how much protein they’re eating. Track everything for a week using an app like Cronometer or MyFitnessPal, and you’ll likely find you’re getting 30-40% less than you assumed.
Build meals around protein first. Instead of asking “what should I eat?” start with “what’s my protein source for this meal?” Then add vegetables, healthy fats, and carbs around that protein centerpiece. This mental shift makes hitting targets much easier than treating protein as one component among many.
Prioritize protein-dense foods. Some foods deliver far more protein per calorie than others:
- Highest density (20-30g protein per 100 calories): chicken breast, turkey, tuna, shrimp, egg whites, whey protein
- High density (15-20g per 100 calories): salmon, lean beef, eggs, Greek yogurt, cottage cheese
- Moderate density (8-15g per 100 calories): tofu, tempeh, lentils, chickpeas, quinoa
If you’re struggling to meet targets, emphasize the highest-density sources.
Use protein supplements strategically. Whole food should be the foundation, but protein powder is a legitimate tool. It’s particularly useful for people with low appetites (older adults, those on GLP-1 medications), athletes with very high needs, busy people who struggle to prepare protein-rich meals, and anyone trying to hit elevated targets on a plant-based diet. Whey, casein, soy, pea, and rice proteins are all well-studied and effective. The “best” protein powder is the one you’ll actually use consistently.
Front-load protein to breakfast. Most people dramatically undereat protein at breakfast (often getting 10-15 grams from cereal and milk) and then try to catch up at dinner. This pattern means muscle protein synthesis is suboptimal for most of the day. Prioritizing 30+ grams at breakfast sets up better protein distribution. The morning protein strategy involves starting each day with eggs, Greek yogurt, or a protein smoothie rather than carb-heavy options.
Common Protein Myths Debunked
Several persistent myths about protein deserve clarification:
“High protein damages kidneys.” There is no evidence this is true for people with healthy kidneys. The concern originates from recommendations for people with pre-existing kidney disease, who do need to moderate protein intake. For healthy individuals, high protein intake is safe and does not cause kidney damage. Multiple systematic reviews have confirmed this.
“You can only absorb 30g of protein per meal.” False. Your body can digest and absorb essentially all the protein you eat; amino acids don’t pass through unused. The 30-40g threshold is about maximizing muscle protein synthesis, not absorption. Eating more protein gets absorbed and used for energy, immune function, enzyme production, and other purposes; it just doesn’t stimulate additional muscle building.
“Plant protein is inferior and can’t build muscle.” Plant proteins work well for muscle building; you just need slightly more total protein and should vary sources to ensure complete essential amino acid intake. Vegetarian and vegan athletes can absolutely meet protein needs and build muscle. Soy protein, in particular, has been shown to support muscle building similarly to animal protein when total intake is adequate.
“More protein is always better.” There are diminishing returns beyond roughly 2.2g/kg for most people. Additional protein beyond this level doesn’t provide additional muscle-building or health benefits in most research. The extra calories from protein have to go somewhere, and while protein is less easily stored as fat than carbohydrates, excess is still excess.
The Bottom Line
Protein requirements are more individual and more elevated than the outdated RDA suggests. The old minimum was designed to prevent deficiency in sedentary laboratory subjects; it was never intended as an optimization target for active people, older adults, those losing weight, or anyone pursuing health rather than just survival.
For most healthy adults, optimal protein intake falls in the range of 1.2-2.2g/kg body weight (0.55-1.0g per pound), with your specific needs depending on age, activity level, goals, and circumstances. Older adults need more than younger adults. Active people need more than sedentary people. Those losing weight need more than those maintaining. Those on GLP-1 medications need to prioritize protein above nearly everything else.
Quality matters alongside quantity. Complete proteins with adequate leucine content support muscle building more effectively than incomplete proteins. Distribution matters too: spreading protein across multiple meals optimizes muscle protein synthesis throughout the day.
Next Steps:
- Calculate your target: multiply your weight in pounds by 0.7-1.0 (or kg by 1.5-2.2) based on your goals and activity level
- Track your actual intake for one week to identify gaps
- Restructure meals to put protein first
- Add a protein-rich breakfast if you currently skimp in the morning
- Consider a pre-bed protein source (Greek yogurt, cottage cheese) for overnight muscle support
Sources: American Journal of Clinical Nutrition, Journal of the International Society of Sports Nutrition position stand, Journal of Nutrition Health and Aging, Nutrients 2019 systematic review on older adults, GLP-1 medication clinical data, protein distribution and muscle protein synthesis research from University of Texas and McMaster University.





