For decades, the treatment paradigm for Post-Traumatic Stress Disorder focused almost exclusively on cognitive interventions: talk therapy, cognitive processing therapy, prolonged exposure, and medication to manage symptoms. The underlying assumption was that trauma was fundamentally a disorder of thoughts and memories, something that could be resolved by talking through experiences and restructuring cognitive patterns. Yet many trauma survivors found that despite years of therapy, their bodies continued to react as though the threat was still present. Hearts raced during benign situations. Muscles tensed at unexpected sounds. Sleep remained elusive. The mind might understand that the trauma was past, but the body hadn’t received the message.
Groundbreaking work from researchers and clinicians like Dr. Bessel van der Kolk, whose book The Body Keeps the Score has transformed trauma treatment, has revealed why purely cognitive approaches often fall short. Trauma is physiological, not just psychological. It gets stored in the body, in the nervous system, in patterns of muscle tension and breath holding that persist long after the traumatic event ends. The brain’s fear circuitry, particularly the amygdala and the body’s stress response systems, becomes hyperactivated and remains stuck in threat-detection mode regardless of what the conscious mind believes.
This understanding has elevated exercise from an “optional wellness add-on” to a core component of comprehensive PTSD treatment. Movement offers a bottom-up pathway to healing that complements top-down cognitive approaches. By engaging the body directly, exercise can access and help process traumatic stress in ways that words alone often cannot reach. The evidence base has grown substantial: multiple randomized controlled trials now demonstrate that exercise reduces PTSD symptoms with effect sizes comparable to established psychotherapies. For the approximately 7-8% of Americans who will experience PTSD at some point in their lives, understanding how exercise contributes to healing offers an accessible, empowering addition to their recovery toolkit.
The Stuck Stress Response: Understanding PTSD Physiology
To understand how exercise helps PTSD, you first need to understand what PTSD does to the body. The traumatic stress response is not a character flaw or a failure of willpower; it’s a physiological state that becomes entrenched through neural learning and hormonal dysregulation.
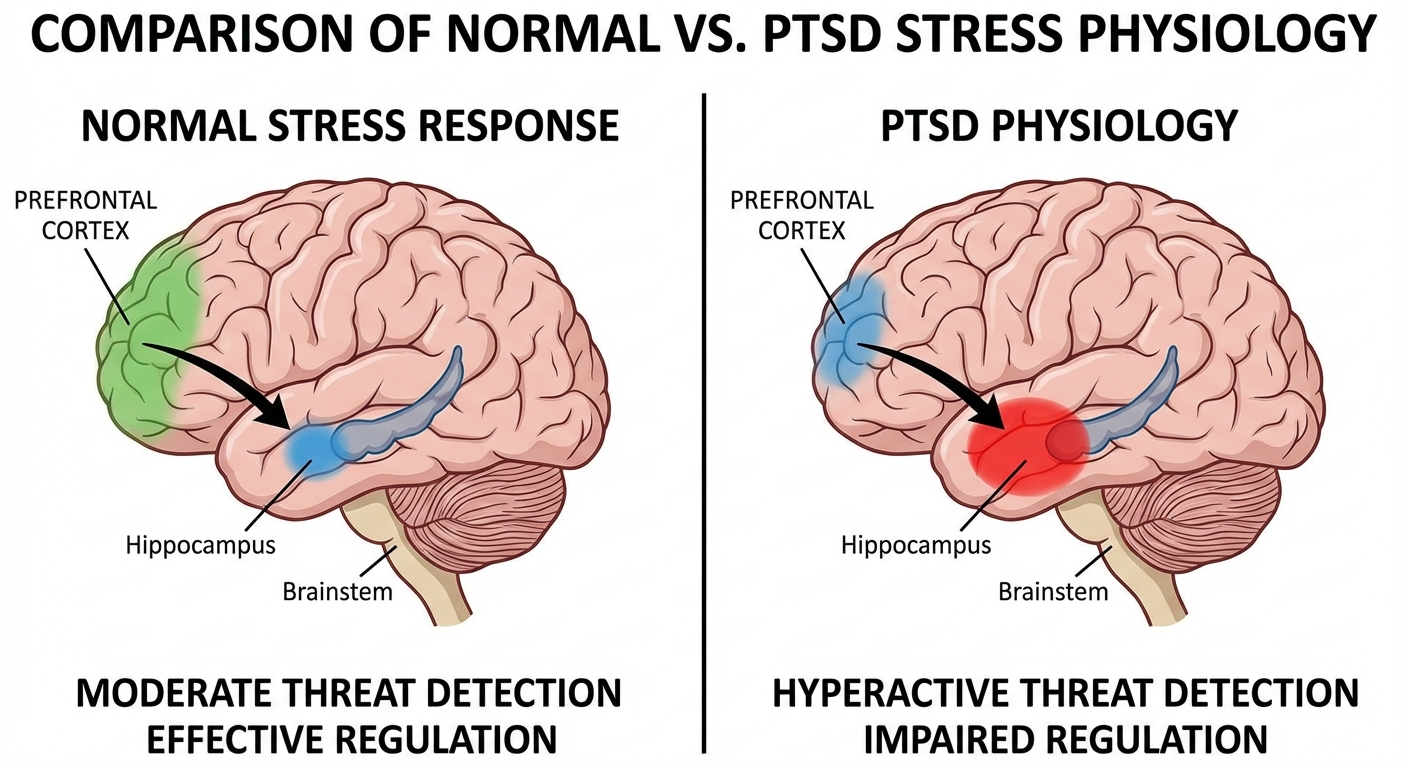
During a traumatic event, the amygdala, the brain’s threat-detection center, activates the hypothalamic-pituitary-adrenal (HPA) axis and the sympathetic nervous system. Stress hormones flood the body: cortisol, adrenaline, noradrenaline. Heart rate increases, breathing becomes shallow and rapid, muscles tense for fight or flight. Blood flow redirects from digestive and reproductive organs to large muscle groups. The prefrontal cortex, responsible for rational thought and executive function, partially shuts down as the survival brain takes over.
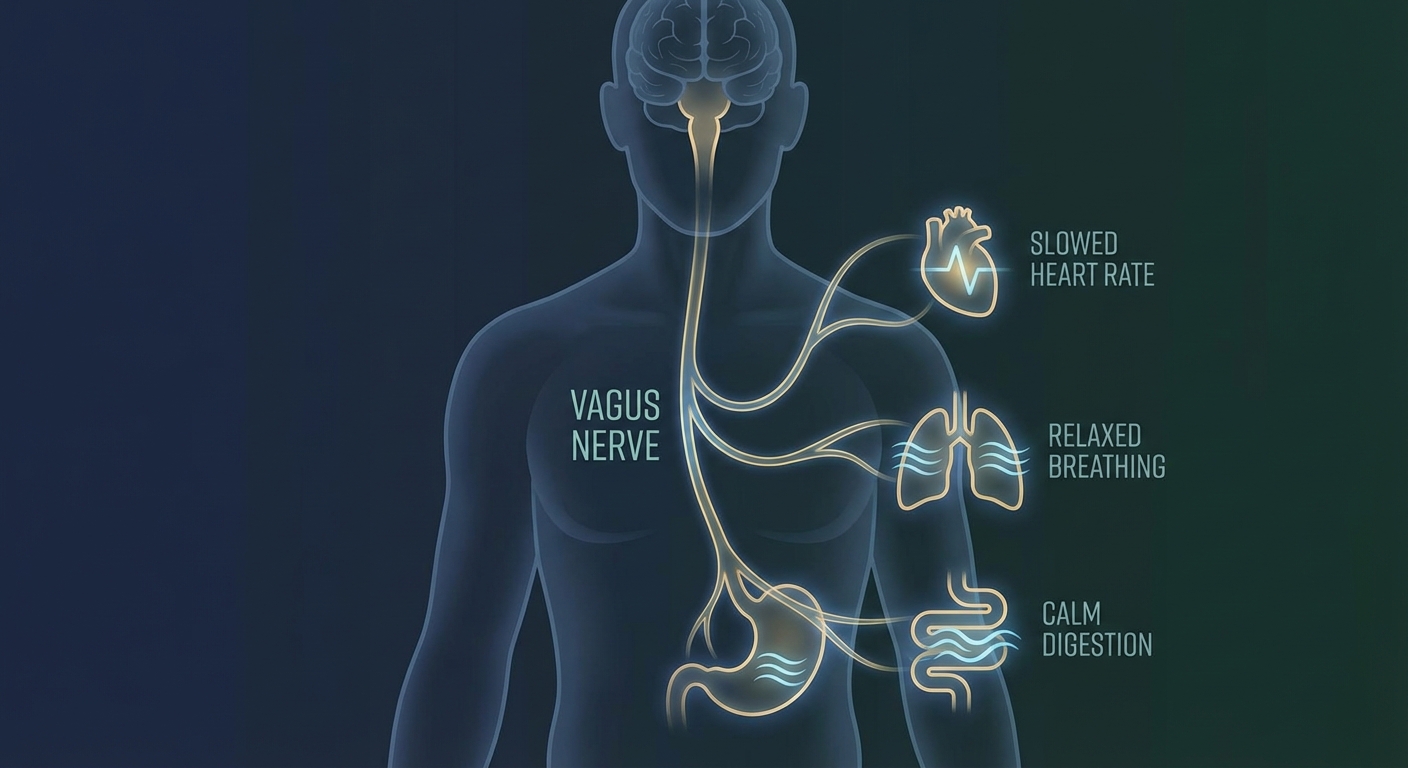
In healthy stress responses, this activation resolves once the threat passes. The parasympathetic nervous system engages, cortisol levels normalize, and the body returns to baseline. But in PTSD, this resolution doesn’t occur. The nervous system remains stuck in a threat-detection state, hypervigilant for danger that no longer exists. The amygdala stays hyperactive, the prefrontal cortex remains inhibited, and the body continues producing stress hormones in response to triggers that objectively pose no threat.
This stuck state manifests in the hallmark symptoms of PTSD: hyperarousal (exaggerated startle response, difficulty sleeping, irritability), intrusion (flashbacks, nightmares, intrusive memories), avoidance (steering clear of reminders, emotional numbing), and negative alterations in cognition and mood. The body is constantly preparing for a fight or flight response that never comes, depleting resources and preventing the rest and repair that normal function requires.
Interoceptive Exposure: Retraining the Body’s Panic Response
One of the cruelest aspects of PTSD is that the body’s natural sensations become triggers. A racing heart from walking up stairs can feel terrifyingly similar to the racing heart of a panic attack or a flashback. Heavy breathing from exertion mimics the respiratory pattern of acute fear. This is interoceptive conditioning: the internal sensations of physiological arousal have become associated with danger, creating a feedback loop where normal bodily responses to exercise trigger the same fear response as the original trauma.
Exercise provides controlled interoceptive exposure, a gradual, voluntary way to retrain the brain’s interpretation of bodily sensations. By deliberately inducing elevated heart rate, heavy breathing, and muscle tension in safe environments, like a gym, a running trail, or a yoga studio, the brain begins to decouple these physical sensations from traumatic memory. You experience your heart beating at 150 bpm and nothing bad happens. You feel your breath becoming rapid and survive without catastrophe. Over time, the sensations lose their power to trigger fear responses.
Dr. Jasper Smits, a clinical psychologist at the University of Texas whose research focuses on exercise and anxiety disorders, has demonstrated that regular aerobic exercise reduces anxiety sensitivity, the fear of anxiety-related sensations. This reduction appears to mediate some of exercise’s effects on PTSD symptoms. As people become more comfortable with the physical sensations of arousal, triggers lose their power, and the hyperarousal symptoms of PTSD diminish.
The key is that the exposure must be voluntary and controlled. Being forced to experience elevated heart rate in an unsafe or unpredictable environment would reinforce the trauma association. But choosing to elevate your heart rate through exercise, in an environment you control, with the ability to stop at any time, creates new associations: arousal can be safe, chosen, and even pleasurable. This relearning happens below conscious awareness, in the same subcortical systems where the trauma is encoded.
BDNF: Neuroplasticity and Brain Repair
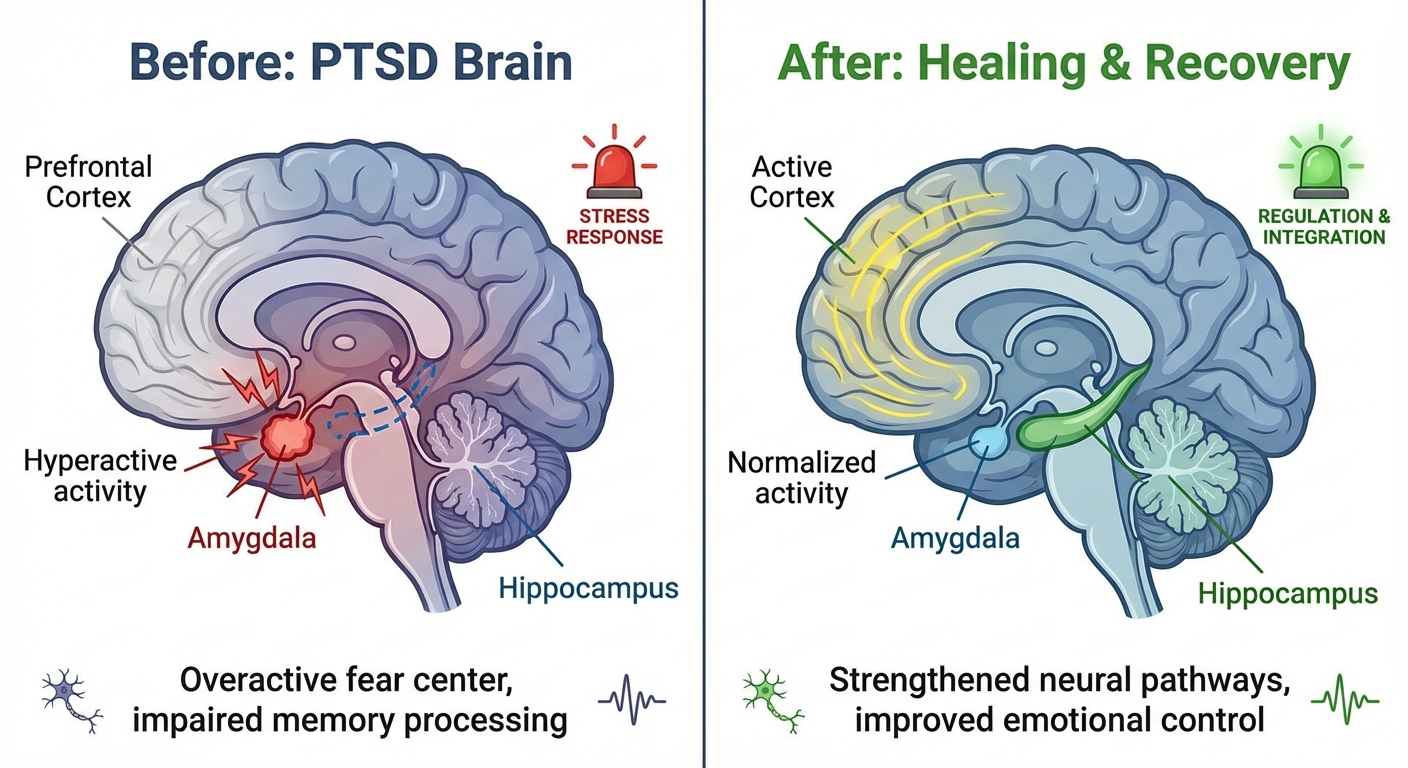
PTSD is associated with measurable changes in brain structure, particularly in the hippocampus, the region responsible for memory consolidation and emotional context. Neuroimaging studies consistently show reduced hippocampal volume in people with PTSD compared to matched controls. This atrophy helps explain a hallmark symptom: traumatic memories feel “present” rather than “past.” The hippocampus normally timestamps memories, placing them in historical context. When hippocampal function is compromised, the brain loses its ability to distinguish between “that happened then” and “this is happening now,” which is why flashbacks feel so vivid and immediate.
Aerobic exercise triggers the release of Brain-Derived Neurotrophic Factor (BDNF), often described as “Miracle-Gro” for neurons. BDNF promotes neurogenesis (the growth of new brain cells), enhances synaptic plasticity (the ability of neural connections to strengthen and change), and supports the survival of existing neurons. The hippocampus is particularly responsive to BDNF, and multiple studies have shown that regular aerobic exercise increases hippocampal volume in both healthy adults and those with depression or anxiety disorders.
For PTSD specifically, the implications are significant. A healthier, larger hippocampus can more effectively categorize traumatic memories as past events that are over rather than ongoing threats. Research from Dr. Kirk Erickson at the University of Pittsburgh has demonstrated that even moderate aerobic exercise (walking 40 minutes three times weekly for one year) increased hippocampal volume by approximately 2% in older adults, essentially reversing age-related shrinkage by one to two years. While direct studies on hippocampal recovery in PTSD through exercise are still accumulating, the neurobiological mechanism is promising.
The BDNF response to exercise is dose-dependent but doesn’t require extreme intensity. Moderate aerobic exercise (50-75% of maximum heart rate) sustained for 30 or more minutes produces robust BDNF elevation. High-intensity interval training may produce even greater acute BDNF release, though the optimal protocol for PTSD recovery specifically remains under investigation.
Bilateral Stimulation: The Rhythm of Healing
Activities involving rhythmic, bilateral movement, simultaneously engaging both sides of the body in alternating patterns, appear to have unique benefits for processing trauma. This concept emerged from EMDR (Eye Movement Desensitization and Reprocessing), a well-established trauma therapy that uses back-and-forth eye movements to facilitate processing of traumatic memories. The bilateral stimulation is thought to enhance communication between brain hemispheres and activate neural networks involved in memory processing and integration.
Running, walking, swimming, cycling, and rowing all involve this rhythmic left-right alternation. Each step, each stroke, each pedal revolution engages both hemispheres of the brain in coordinated sequence. Many trauma survivors report that the rhythmic cadence of a long run allows them to process thoughts and emotions that are too difficult to sit with in stillness. The movement seems to create a “trance-like” state where traumatic material can surface, be acknowledged, and begin to integrate without overwhelming the nervous system.
Dr. Bessel van der Kolk has written about the special value of rhythmic activities for trauma recovery. “Rhythm is essential for establishing the sense of time and sequence that trauma disrupts,” he notes. “Rhythmic movement helps reestablish the natural rhythms of the nervous system that trauma throws off.” The steady beat of footfall on trail, the circular motion of pedaling, the alternating reach of swimming strokes all provide external rhythmic structure that may help stabilize internal rhythmic processes.
This doesn’t mean that bilateral activities are the only helpful exercise for PTSD. Strength training, yoga, martial arts, and team sports all show benefits in research. But for those who find that running or walking helps them “think through” difficult material, the bilateral stimulation hypothesis offers a neurobiological explanation for what many trauma survivors intuitively discover.
A Trauma-Informed Approach to Exercise
For someone with PTSD, jumping into intense exercise can backfire. A loud, crowded gym with mirrors and strangers may trigger hypervigilance. High-intensity workouts that push heart rate to extremes may overwhelm the nervous system rather than gradually retrain it. The goal is safety and gradual exposure, not intensity and performance.
Control the environment. Choose workout settings that feel safe. For many trauma survivors, this means outdoor trails, home workouts, or quiet gym times rather than crowded fitness classes. Avoid environments with unpredictable noises, crowds of strangers, or mirrors that create self-consciousness. The ability to leave at any time is essential; feeling trapped amplifies the threat response.
Start with low-intensity movement. Walking is an underrated trauma recovery tool. It’s bilateral, rhythmic, accessible, and low-intensity enough to remain below the threshold that triggers panic. A 20-minute walk produces BDNF elevation, provides interoceptive exposure to mild arousal, and can be done in environments you control. Build from walking to jogging only when walking feels consistently safe and grounding.
Focus on sensation rather than performance. Instead of counting reps, tracking pace, or monitoring metrics, direct attention to bodily sensations: how your feet feel hitting the ground, how air moves in and out of your lungs, how your muscles engage and release. This somatic mindfulness anchors you in present-moment bodily experience, counteracting the dissociation that often accompanies trauma and building the interoceptive awareness that trauma disrupts.
Prioritize consistency over intensity. A 20-minute walk every day is infinitely more valuable than one intense session weekly that leaves you overwhelmed. You’re rebuilding trust with your body, not punishing it. The nervous system responds to repeated signals of safety, not occasional signals of intensity. Gradual, consistent practice allows the body to slowly recalibrate its baseline.
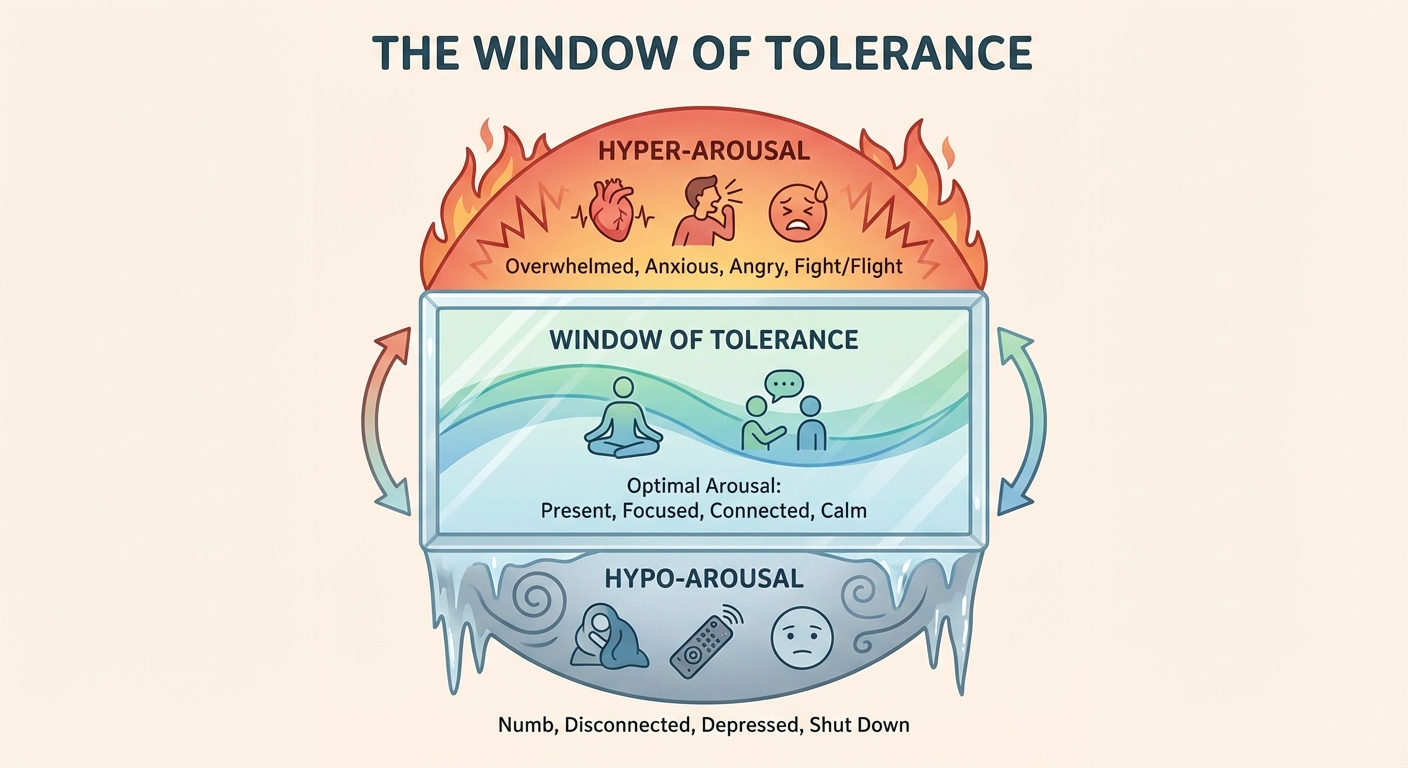
Recognize window of tolerance. Dr. Dan Siegel’s concept of the “window of tolerance” describes the zone of arousal within which a person can function effectively. Below the window is hypoarousal (shutdown, numbness, dissociation); above it is hyperarousal (panic, rage, overwhelm). Exercise for PTSD recovery should keep you within or gently expand this window, not blast you above it. If exercise consistently triggers flashbacks, panic, or dissociation, scale back intensity or duration and consider working with a trauma-informed fitness professional.
Integrating Exercise with Other Treatment
Exercise is not a replacement for trauma therapy. It’s a complement that works through different mechanisms and can enhance the effectiveness of other treatments. The most robust outcomes in PTSD research typically involve multi-modal approaches: therapy, medication when appropriate, social support, and lifestyle factors including exercise, sleep, and nutrition.
Exercise may enhance therapy outcomes by improving the neuroplasticity that allows traumatic memories to be reprocessed. The BDNF elevation from exercise creates a brain state more receptive to new learning, potentially amplifying the effects of cognitive processing therapy or EMDR. Some clinicians are experimenting with scheduling exercise sessions immediately before or after therapy sessions to capitalize on this enhanced plasticity window.
For veterans and others with PTSD who have experienced medication side effects or prefer non-pharmacological approaches, exercise provides an evidence-based option that many find empowering. Unlike taking a pill, exercise is something you do actively, which can restore a sense of agency that trauma often destroys. The act of choosing to move, of proving to yourself that your body can do hard things and survive, rebuilds the fundamental trust in yourself that trauma erodes.
For those seeking additional resources, our guide on tactical breathing techniques covers breathing practices that complement exercise for nervous system regulation, while the article on walking and its mental health benefits explores how even gentle movement provides a foundation for trauma recovery.
The Bottom Line
Healing from trauma is a whole-body process. The body keeps the score, but the body can also be the pathway to recovery. By using movement to retrain interoceptive responses, boost neuroplasticity through BDNF, engage rhythmic bilateral stimulation, and reclaim ownership of physical sensations, exercise transforms the body from an enemy into an ally.
The evidence is substantial and growing: exercise reduces PTSD symptoms with effect sizes comparable to established psychotherapies. It works through mechanisms that cognitive approaches don’t access, providing bottom-up regulation that complements top-down processing. And it’s accessible, affordable, and can be done on your own terms, in environments you control, at intensities you choose.
For trauma survivors who have spent years feeling betrayed by their bodies, learning to work with the body rather than against it can be revolutionary. Exercise isn’t just about fitness; it’s about reintegration, healing the split between mind and body that trauma creates. One step, one breath, one movement at a time, you rebuild the connection to yourself that trauma tried to destroy.
If you’re struggling with PTSD, please work with a mental health professional. The strategies in this article are supportive practices, not replacements for professional treatment. If you’re experiencing persistent symptoms, suicidal thoughts, or severe impairment, reach out to a trauma-specialized therapist, psychiatrist, or crisis service.
Trauma-Informed Exercise Protocol:
- Start with daily walking (20-30 minutes) in a safe, controlled environment
- Focus on bodily sensations rather than performance metrics
- Maintain intensity within your window of tolerance (mild exertion, not panic)
- Progress gradually: walk → jog → run as each level feels safe
- Consider bilateral rhythmic activities (swimming, cycling, rowing)
- Schedule exercise to complement, not replace, trauma therapy
Sources: The Body Keeps the Score (Dr. Bessel van der Kolk), University of Texas anxiety sensitivity research (Dr. Jasper Smits), University of Pittsburgh hippocampal volume studies (Dr. Kirk Erickson), EMDR and bilateral stimulation research, American Psychological Association PTSD treatment guidelines, VA/DoD Clinical Practice Guidelines for PTSD, Journal of Clinical Psychology exercise and PTSD meta-analyses.