Five years ago, when collagen supplements first flooded the wellness market, the scientific establishment dismissed them as expensive nonsense. The argument seemed airtight: your digestive system breaks all proteins down into individual amino acids, so eating collagen is no different from eating any other protein. Your body doesn’t know whether those amino acids came from collagen peptides or chicken breast; it just reassembles them according to its own priorities. The collagen you swallow becomes whatever your body needs, not necessarily new collagen in your skin or joints.
This critique made sense based on classical protein biochemistry. It was also, as we now understand, incomplete. The research that accumulated between 2020 and 2025 revealed something the early critics missed: hydrolyzed collagen peptides don’t fully break down during digestion. Specific di- and tri-peptide fragments survive the stomach and appear intact in the bloodstream, where they act as signaling molecules rather than simple building blocks. They don’t just provide raw materials; they tell your cells to get to work.
This distinction transforms the conversation from “does collagen work?” to “for what conditions, at what doses, does the evidence support collagen supplementation?” The answer, as of late 2025, is more nuanced and more positive than either enthusiastic marketers or skeptical scientists initially claimed.
The Mechanism: Signaling, Not Just Building Blocks
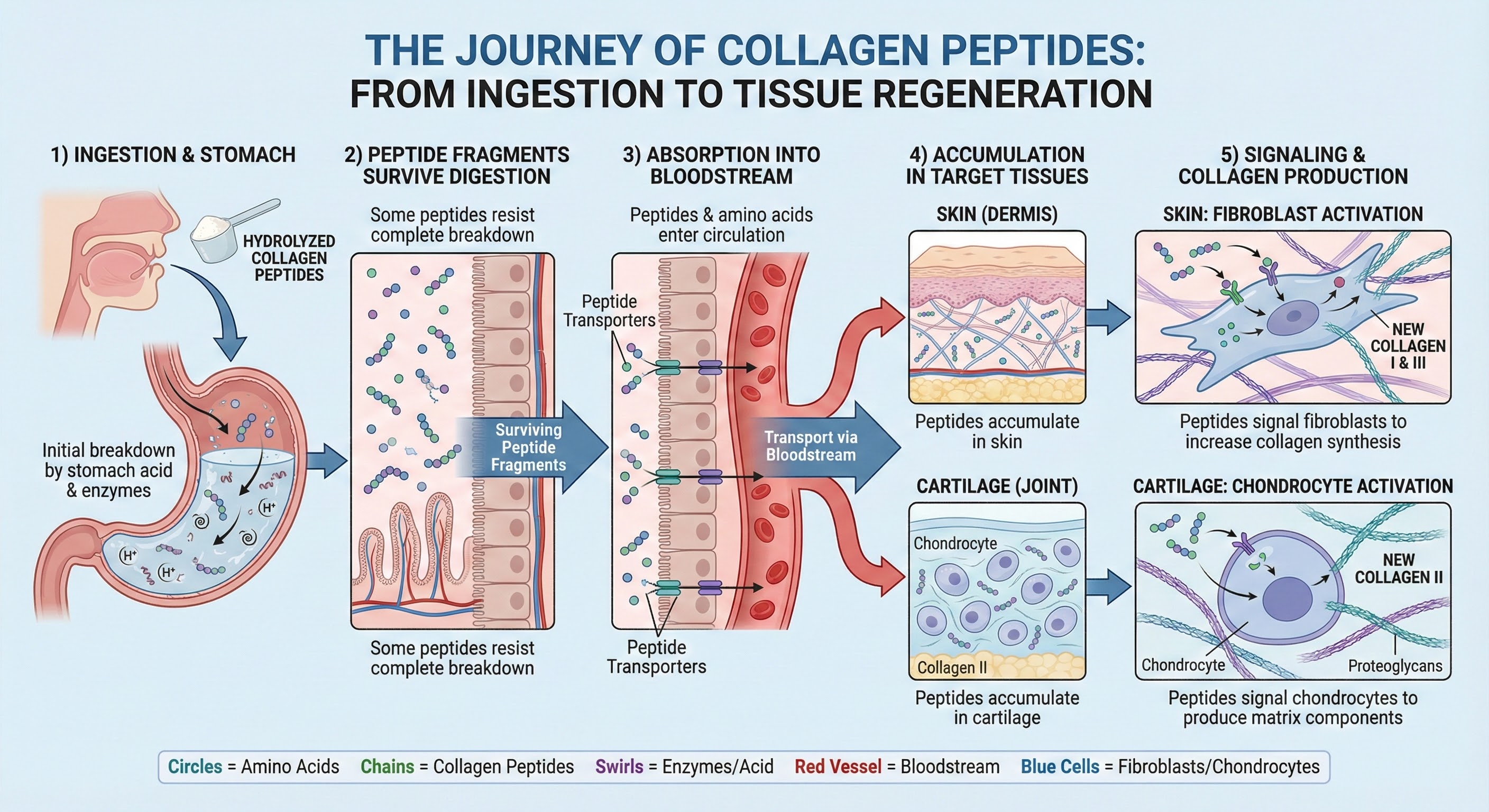
Understanding why collagen supplements might work requires revisiting what happens after you swallow a scoop of collagen powder. Hydrolyzed collagen, the form used in supplements, has been enzymatically broken into smaller peptide chains before you ever consume it. This pre-digestion creates fragments small enough to survive the stomach’s acidic environment and pass through the intestinal wall into the bloodstream.
Research using radioactively labeled collagen peptides has tracked where these fragments go after ingestion. Studies published in the Journal of Agricultural and Food Chemistry demonstrated that hydroxyproline-containing peptides (a signature of collagen) appear in blood within 1-2 hours of consumption and accumulate preferentially in cartilage, bone, and skin tissue. This tissue-specific accumulation suggests active transport mechanisms, not random distribution.
More importantly, these peptides appear to function as signaling molecules. When collagen-specific peptide fragments appear in blood, your body interprets them as evidence that collagen is breaking down somewhere and responds by upregulating collagen synthesis. Fibroblasts in the skin, chondrocytes in cartilage, and osteoblasts in bone all increase their production of new collagen matrix in response to these signals. It’s a biological “false alarm” that triggers a real repair response.
This mechanism explains why collagen supplements might offer benefits that generic protein sources don’t. Whey protein or chicken breast provides amino acids that your body can use for any purpose, allocated according to priority. Collagen peptides provide both amino acids and a specific stimulus for collagen production in target tissues. The signal matters as much as the substrate.
Skin Health: The Strongest Evidence
The dermatological applications of collagen supplementation have the most robust research support. Multiple randomized controlled trials and several meta-analyses have now examined collagen’s effects on skin aging markers, consistently finding benefits that exceed placebo.
A 2019 meta-analysis published in the Journal of Drugs in Dermatology pooled data from 11 randomized controlled trials encompassing 805 participants. The analysis found that collagen supplementation significantly improved skin hydration, elasticity, and wrinkle appearance compared to placebo, with effects becoming apparent after 4-12 weeks of daily supplementation. The effect sizes were modest but statistically significant and clinically noticeable to participants.
A 2021 systematic review in the International Journal of Dermatology examined 19 studies and reached similar conclusions, finding “favorable results for short and long-term use of oral collagen supplements for wound healing and skin aging.” The authors noted that while study quality varied, the consistency of positive findings across different populations, dosages, and collagen sources suggested a genuine biological effect rather than publication bias.
The mechanism appears to involve both direct and indirect pathways. Collagen peptides stimulate fibroblast activity, increasing production of new collagen and elastin fibers in the dermis. They also increase hyaluronic acid production, improving skin hydration. Additionally, some evidence suggests collagen peptides have antioxidant properties that protect existing collagen from degradation.
Practical parameters from the research: most positive studies used doses of 2.5-10 grams of hydrolyzed collagen daily, with benefits appearing after 4-8 weeks and continuing to improve over 3-6 months of consistent use. Marine collagen (Type I) and bovine collagen (Types I and III) both show efficacy for skin outcomes. Lower molecular weight peptides (around 3,000 daltons) appear to have better bioavailability than larger fragments.
Joint Health: Moderate Evidence with Specific Applications
The orthopedic evidence for collagen is more nuanced than dermatological findings. Effects vary substantially based on the underlying condition, the type of collagen used, and the specific outcome measured.
For osteoarthritis, the evidence is moderately positive. A 2017 meta-analysis in the British Journal of Sports Medicine examined data from 41 studies and found that collagen supplementation produced small but statistically significant improvements in pain and function compared to placebo. A 2023 Cochrane review took a more cautious view, concluding that while collagen showed promise, the evidence base had significant limitations including risk of bias and heterogeneity between studies.
For activity-related joint pain in athletes without diagnosed arthritis, the evidence is stronger. A landmark Penn State study published in Current Medical Research and Opinion followed 147 athletes over 24 weeks and found that those taking 10g of collagen hydrolysate daily reported significantly less joint pain during activity compared to placebo. The study specifically recruited athletes with activity-related joint pain but no diagnosed joint disease, a population particularly relevant for supplement users.
The mechanism for joint benefits likely differs from skin benefits. Type II collagen (found primarily in cartilage) may work partly through an immune-modulating mechanism called oral tolerance, where small doses of collagen peptides downregulate the autoimmune inflammation that contributes to cartilage degradation. Undenatured Type II collagen (UC-II), a specific formulation that preserves collagen structure, has shown particular promise for this application at doses as low as 40mg daily.
Type I and III collagen (from bovine or marine sources) may support cartilage through a different pathway, providing substrate and signaling for the extracellular matrix that cushions and lubricates joints. These forms typically require higher doses (10g+) and show benefits in studies focused on structural cartilage support rather than inflammation reduction.
The Amino Acid Advantage: Glycine and Proline
Even setting aside the signaling mechanism, collagen supplements provide an amino acid profile that’s genuinely difficult to obtain from modern diets. Collagen is approximately 33% glycine, 10% proline, and contains significant hydroxyproline, amino acids that most people under-consume.
Glycine is the limiting factor in this picture. Research published in the Journal of Bioscience and Bioengineering estimated that the average adult requires approximately 10 grams of glycine daily for optimal collagen synthesis, glutathione production, and other metabolic functions. The typical Western diet provides only 2-3 grams. This gap can be closed either by consuming glycine-rich foods (bone broth, skin, connective tissue) or through supplementation.
The glycine shortfall matters because glycine is essential for multiple biological processes beyond collagen production. It’s a precursor to glutathione, the body’s master antioxidant. It serves as an inhibitory neurotransmitter that supports sleep quality. It’s required for creatine synthesis and plays roles in DNA methylation and detoxification pathways. When glycine supply is limited, the body prioritizes essential functions and potentially shortchanges collagen production.
This biochemical reality explains why some people experience noticeable benefits from collagen supplementation even if the signaling mechanism were entirely theoretical. Simply providing adequate glycine and proline, which the modern muscle-meat-centric diet doesn’t supply, could theoretically improve collagen production in people who were functionally deficient in these conditionally essential amino acids.
A 10-gram serving of hydrolyzed collagen provides approximately 3.3 grams of glycine and 1 gram of proline. Combined with dietary intake, this brings most people much closer to estimated requirements and may represent genuine nutritional repletion rather than pharmacological supplementation.
The Vitamin C Connection: Essential but Often Overlooked
Collagen synthesis absolutely requires vitamin C as a cofactor. The enzymes that cross-link collagen fibers into stable, functional structures (prolyl hydroxylase and lysyl hydroxylase) cannot function without adequate ascorbic acid. This requirement is so strict that severe vitamin C deficiency causes scurvy, a disease characterized by collagen breakdown throughout the body.
This biochemistry has practical implications for collagen supplementation. Taking collagen peptides without adequate vitamin C provides signals and substrates for collagen production but limits the efficiency of the synthesis process. Some research suggests that co-administration of collagen with vitamin C enhances benefits beyond either supplement alone.
A 2018 study in the Journal of Cosmetic Dermatology found that women taking a combination of hydrolyzed collagen and vitamin C showed greater improvements in skin elasticity and hydration than those taking either supplement alone. While this was a single study with limitations, the biochemical rationale for combination is solid.
Many commercial collagen supplements now include vitamin C for this reason. If yours doesn’t, ensure you’re meeting vitamin C requirements through diet (citrus fruits, bell peppers, strawberries, broccoli) or supplementation. Taking collagen with a meal containing vitamin C sources, or simply adding a squeeze of lemon to your collagen drink, supports optimal utilization.
Types, Sources, and Quality Considerations
Not all collagen supplements are equivalent. Understanding the differences helps match products to goals and avoid low-quality options.
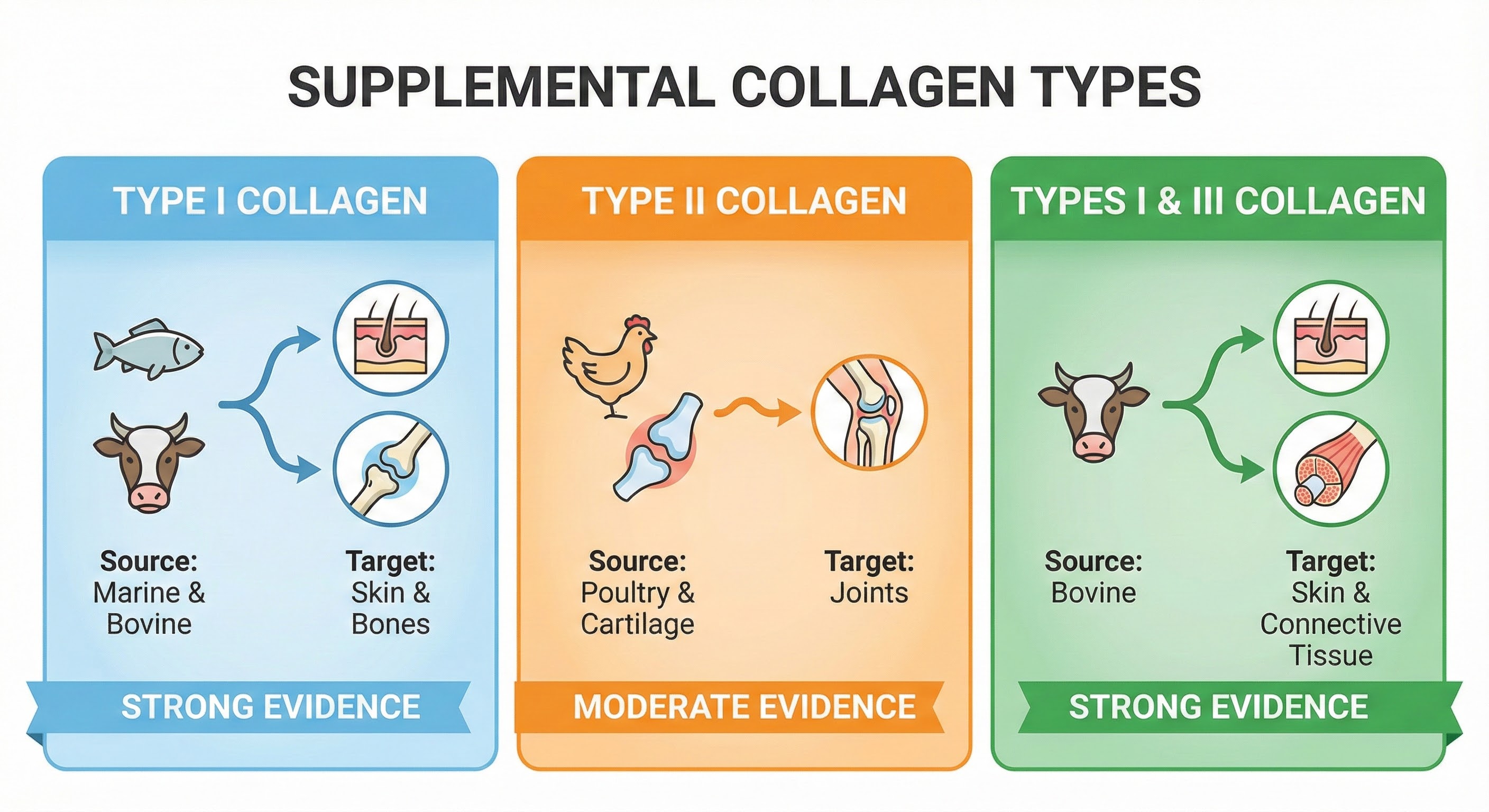
Type I collagen is the most abundant type in the human body, found primarily in skin, bones, tendons, and connective tissue. Marine collagen (from fish) is almost entirely Type I and is prized for smaller peptide size and potentially better absorption. Bovine collagen contains primarily Types I and III.
Type II collagen is found primarily in cartilage and is the main component of the flexible tissues that cushion joints. Chicken-derived collagen is the primary source for Type II supplements. Undenatured Type II collagen (UC-II) is a specific preparation that preserves collagen structure for immune-modulating effects at low doses.
Type III collagen is found alongside Type I in skin and blood vessels. Bovine sources typically provide both Types I and III together.
For skin health, marine or bovine collagen (Type I or I/III) at 2.5-10g daily shows the best evidence. For joint health, the picture is more complex: bovine/marine collagen at higher doses (10g+) for cartilage matrix support, or UC-II at low doses (40mg) for inflammation-related joint issues. Some people stack both approaches for comprehensive joint support.
Quality indicators include third-party testing for heavy metals (particularly relevant for marine collagen), hydrolysis to appropriate molecular weight (2,000-5,000 daltons for optimal absorption), and sourcing from pasture-raised or wild-caught animals. “Collagen peptides” and “hydrolyzed collagen” are essentially synonymous and indicate appropriate processing. Gelatin is a less-processed form with larger molecular weight and potentially lower bioavailability.

What the Evidence Doesn’t Support
Research rigor requires acknowledging limitations alongside positive findings. Several popular claims about collagen lack solid evidentiary support.
Hair growth: While collagen provides amino acids that support hair structure, direct evidence that collagen supplementation improves hair growth or reduces hair loss is weak. A few small studies show promise, but the research base is insufficient to make confident claims. Hair loss has many causes (hormonal, nutritional, genetic) that collagen cannot address.
Gut health: The “leaky gut” claims for collagen are largely theoretical. Glycine and glutamine support intestinal lining, and the logic for collagen supporting gut barrier function is reasonable, but clinical trials demonstrating this benefit in humans are lacking. This area needs more research before claims can be confidently made.
Bone density: Animal studies and some human research suggest collagen may support bone health, but the evidence is preliminary. Collagen provides structural matrix for bones, but the research on supplementation preventing osteoporosis or fractures isn’t mature enough for strong recommendations.
Weight loss: Collagen provides satiating protein and minimal carbohydrates, which could theoretically support weight management as part of a high-protein diet. However, there’s nothing special about collagen for weight loss compared to other protein sources. Any weight loss claims are marketing, not science.
The strongest evidence supports skin hydration, elasticity, and wrinkle reduction; the second-strongest supports activity-related joint pain and potentially osteoarthritis symptoms. Everything else ranges from plausible-but-unproven to speculation.
Practical Recommendations: Who Should Consider Collagen?
Based on the current evidence, collagen supplementation is most defensible for specific populations with specific goals.
Good candidates for collagen supplementation:
- Adults concerned with visible skin aging who want a low-risk intervention with modest but real expected benefits
- Athletes or active individuals experiencing activity-related joint discomfort without diagnosed joint disease
- People with osteoarthritis seeking adjunctive support alongside standard treatments
- Individuals whose diets lack glycine-rich foods (most modern eaters who don’t consume bone broth, organ meats, or skin)
Reasonable dose and timing: 10-15 grams of hydrolyzed collagen (Type I/III for skin, Type I/II/III for comprehensive coverage) taken daily with a vitamin C source. Effects require 4-8 weeks minimum to manifest and continue improving over 3-6 months. For joint-specific issues, consider adding UC-II (40mg) for its distinct mechanism.
Setting realistic expectations: Collagen supplements won’t erase wrinkles, cure arthritis, or produce dramatic transformations. The research shows statistically significant improvements that are noticeable over months but not miraculous. If you’re expecting your skin to look 20 years younger, you’ll be disappointed. If you’re expecting modest improvements in skin hydration and elasticity comparable to good skincare products, the evidence supports that expectation.
The Bottom Line
Collagen has graduated from wellness trend to legitimate supplement category with real, if modest, scientific support. The early criticisms (“it’s just protein”) were oversimplified. Hydrolyzed collagen peptides do behave differently than generic protein, surviving digestion as bioactive signaling molecules that stimulate collagen production in target tissues.
The evidence is strongest for skin health, where multiple meta-analyses support benefits for hydration, elasticity, and wrinkle appearance. Joint health evidence is more mixed but positive for activity-related pain and moderately supportive for osteoarthritis. Claims beyond these areas remain speculative.
Your collagen action plan:
- Identify your goal. Skin health has the strongest evidence. Joint health has moderate evidence. Other claims lack sufficient research.
- Choose appropriate type. Marine or bovine (Type I/III) for skin. Consider adding UC-II for joint inflammation. Type I/II/III combinations provide broad coverage.
- Dose adequately. 10-15 grams daily for most applications. Less is often insufficient to produce noticeable effects.
- Include vitamin C. Either choose a supplement with added vitamin C or take collagen with vitamin C-rich foods.
- Commit to consistency. Benefits appear after 4-8 weeks and continue improving. Give any protocol 3 months before evaluating.
- Maintain realistic expectations. Modest improvements in skin quality and joint comfort, not dramatic transformations.
Collagen isn’t a miracle, but it’s not a hoax either. For specific applications at appropriate doses, it represents one of the better-supported supplements in the crowded wellness market. For a broader look at how nutrition supports skin health from within, explore our guide on nutricosmetics and the role of anti-inflammatory eating.
Sources: Journal of Drugs in Dermatology meta-analysis on skin outcomes (2019), International Journal of Dermatology systematic review (2021), British Journal of Sports Medicine meta-analysis on joint outcomes (2017), Current Medical Research and Opinion on athlete joint pain (Penn State study), Journal of Agricultural and Food Chemistry on collagen peptide bioavailability, Journal of Bioscience and Bioengineering on glycine requirements, Journal of Cosmetic Dermatology on collagen-vitamin C combination (2018), Cochrane review on collagen for osteoarthritis (2023).