
You can build muscle lifting weights at 20-30% of your maximum, the equivalent of warm-up weight for most people. The catch is you need to restrict blood flow to the working muscles using specialized bands or cuffs. What sounds like dangerous gym folklore is actually one of the more robustly researched training methods to emerge in the past two decades.
Blood Flow Restriction (BFR) training, also called occlusion training or KAATSU (after the Japanese inventor Dr. Yoshiaki Sato who developed it in the 1960s), has moved from rehabilitation clinics to mainstream fitness. The research supporting it is surprisingly extensive: multiple systematic reviews and meta-analyses confirm that BFR with light loads produces muscle growth 70-90% as effective as traditional heavy lifting, with dramatically reduced joint stress and recovery demands.
For people with injuries preventing heavy lifting, older adults with joint issues, athletes seeking additional muscle stimulus without additional recovery burden, or anyone traveling with limited equipment, BFR offers an evidence-based approach to building strength that traditional training cannot match. Understanding the mechanisms behind it, the proper protocols, and the legitimate limitations transforms BFR from curiosity to practical tool.
The Physiology of Restriction: Why Light Weights Build Muscle
The core concept of BFR seems counterintuitive: how can partially cutting off blood supply help a muscle grow? The answer lies in manipulating the body’s normal recruitment patterns and metabolic signaling through controlled hypoxia. Under normal circumstances, building significant muscle requires lifting heavy loads, typically 65-85% of your one-rep maximum. This mechanical tension recruits the largest, strongest muscle fibers (Type II fast-twitch fibers) and creates the stimulus for growth.
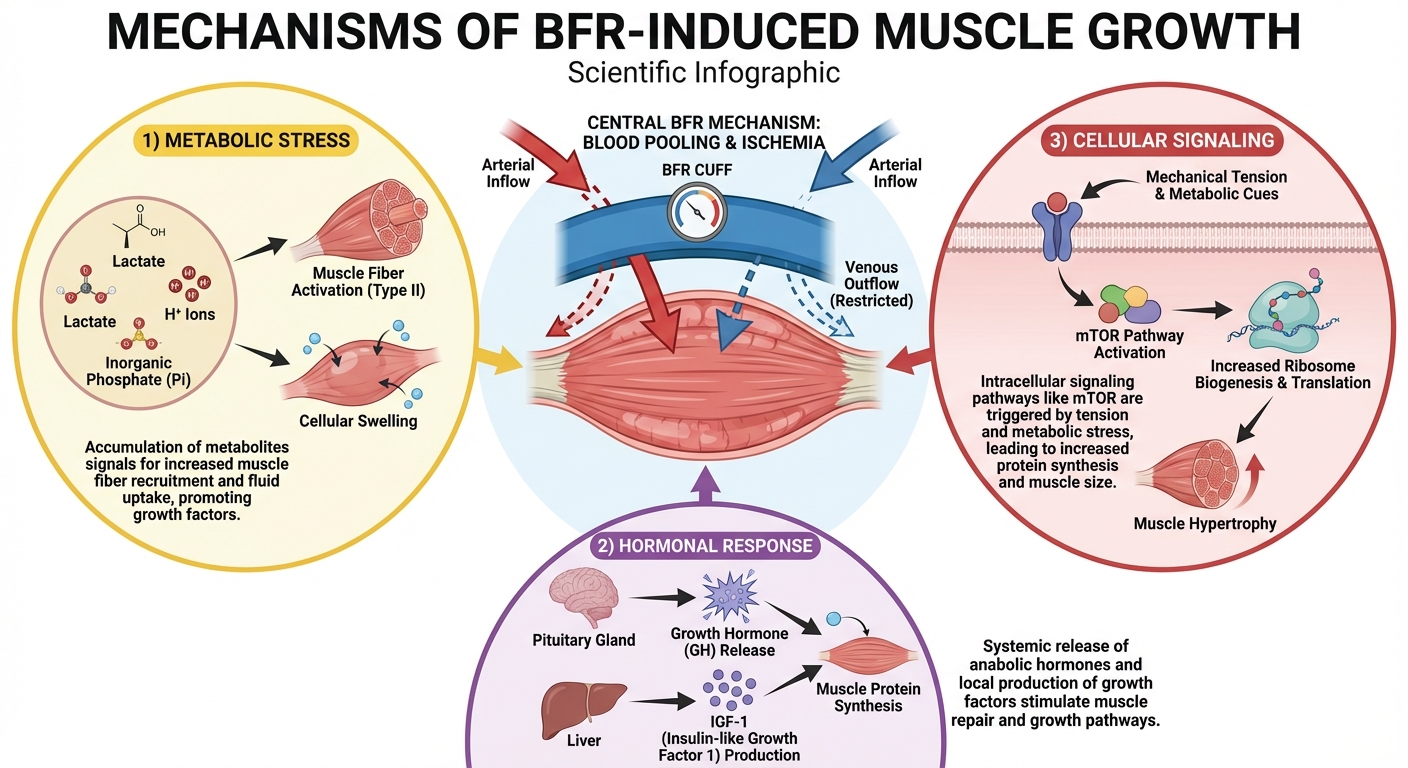
BFR bypasses this mechanical requirement by changing the chemical environment within the muscle. By allowing blood to enter the muscle through arteries but restricting it from leaving through veins, the training creates a hypoxic (low oxygen) environment that forces adaptation. Dr. Jeremy Loenneke, one of the leading BFR researchers at the University of Mississippi, has demonstrated that this restricted blood flow creates three distinct growth signals that don’t require heavy loads.
First, the pooling blood causes metabolic byproducts like lactate and hydrogen ions to accumulate rapidly. This metabolic stress, which normally takes heavy lifting to achieve, signals the brain that the muscle needs to become stronger. Growth hormone levels spike in response, sometimes reaching levels 170% higher than normal exercise according to research published in the Journal of Applied Physiology. Second, fluid accumulates within muscle cells, creating cellular swelling that activates mechanoreceptors and anabolic signaling pathways independent of mechanical tension. This swelling creates the intense “pump” that bodybuilders associate with growth, and in BFR training, this pump actually drives the adaptation.
Third, and perhaps most importantly, the hypoxic conditions force early recruitment of fast-twitch fibers. Normally, your nervous system follows the “size principle” of motor unit recruitment: small, slow-twitch fibers are activated first, with larger fast-twitch fibers only joining when force demands increase. Light weights never recruit fast-twitch fibers under normal conditions. But when oxygen is restricted, slow-twitch fibers fatigue rapidly because they depend heavily on oxygen for energy production. The nervous system is forced to recruit fast-twitch fibers much earlier to maintain force output, creating a stimulus that mimics heavy lifting despite the light load.
The Research Evidence: What Studies Actually Show
Dismissing BFR as a gym gimmick would be easy, but the scientific literature tells a different story. Over the past two decades, hundreds of studies have validated its efficacy across diverse populations. A 2019 meta-analysis in the British Journal of Sports Medicine by Grønfeldt and colleagues, examining 32 randomized controlled trials, concluded that BFR training produces significant increases in both muscle strength and hypertrophy compared to low-load training without restriction.
The comparison to heavy lifting is what makes the research compelling. Traditional strength training requires loads of 65-85% of one-rep maximum to build meaningful muscle. BFR achieves comparable results at 20-40% of one-rep max. A landmark 2012 study by Fahs and colleagues published in Acta Physiologica found that 12 weeks of BFR training at 30% 1RM produced muscle growth statistically similar to traditional training at 70% 1RM. The light-load group built nearly as much muscle while placing dramatically less stress on joints, tendons, and the nervous system.
Strength gains follow similar patterns. A systematic review by Hughes and colleagues in Sports Medicine (2017) found strength increases of 15-40% over 4-12 week periods with BFR training, approaching the gains seen with traditional heavy training. While heavy training still edges out BFR for maximum strength development, the difference is smaller than the load difference would suggest. Getting 80-90% of the results with 30% of the load represents a remarkable efficiency for specific applications.
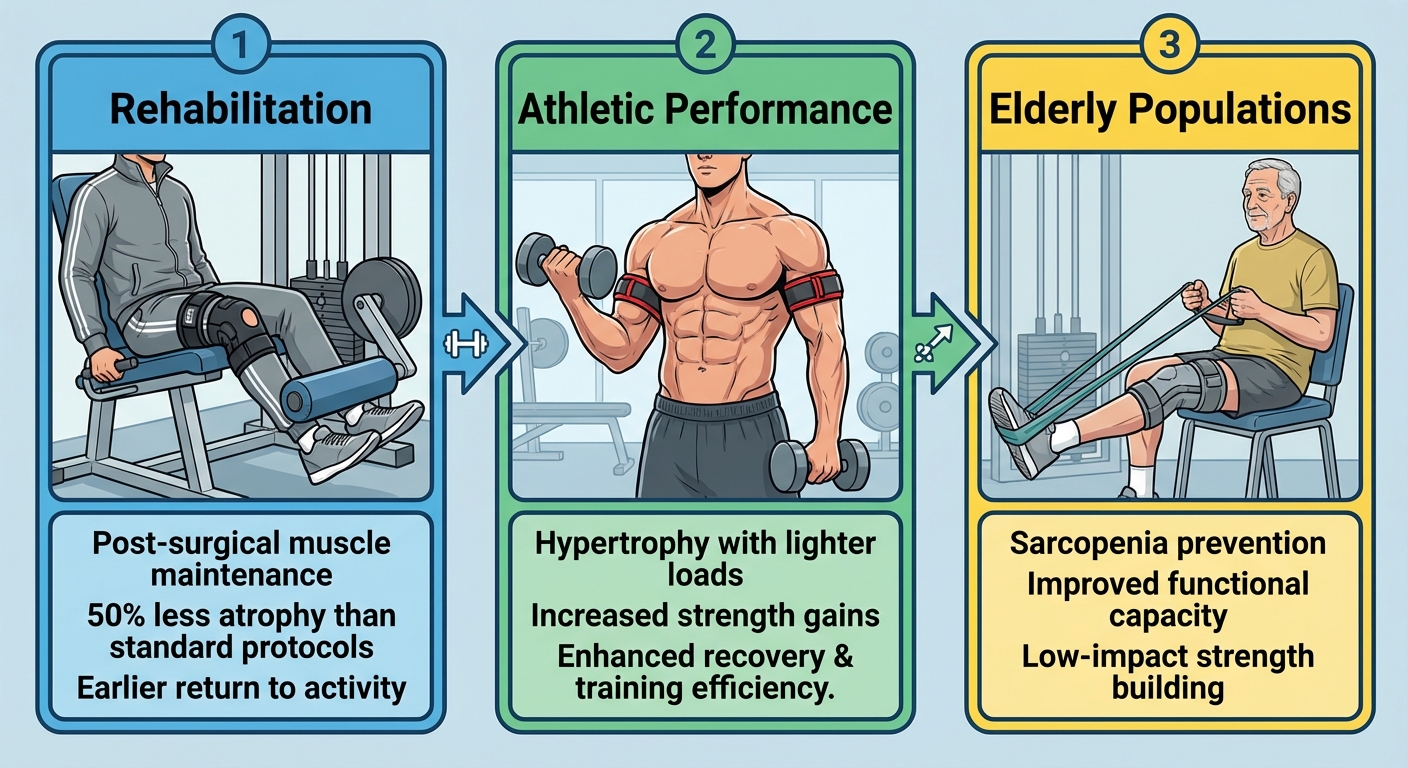
The rehabilitation research is particularly robust because BFR solves a genuine clinical problem. After ACL reconstruction, knee replacement, or shoulder surgery, patients often can’t lift the heavy loads needed to prevent muscle atrophy. Yet atrophy accelerates recovery time and increases re-injury risk. Studies from the American Journal of Sports Medicine show that BFR can reduce quadriceps atrophy by 50% compared to standard post-surgical protocols, allowing patients to maintain muscle while protecting healing tissues. Physical therapist Dr. Nicholas Rolnick, who runs the BFR Pros education company and has published extensively on clinical applications, notes that BFR has become standard practice in many orthopedic rehabilitation settings precisely because it addresses a previously unsolvable problem.
The Proper Protocol: Parameters That Actually Work
Because BFR relies on manipulating blood flow, precision matters more than with standard training. The difference between an effective session and a dangerous one often comes down to pressure settings and timing. This is not as simple as wrapping a resistance band around your arm and curling; the parameters that produce results have been carefully studied.
Equipment matters significantly for both safety and efficacy. Specialized BFR cuffs with pneumatic pressure gauges (like those from brands like Smart Cuffs or Delfi) provide precise, measurable restriction and are the gold standard in research settings. These cuffs are wider (typically 5-10 cm) and apply more even pressure across the limb. Elastic wraps or bands can work but require experience to calibrate tightness appropriately, and narrower bands concentrate pressure in ways that increase nerve impingement risk.
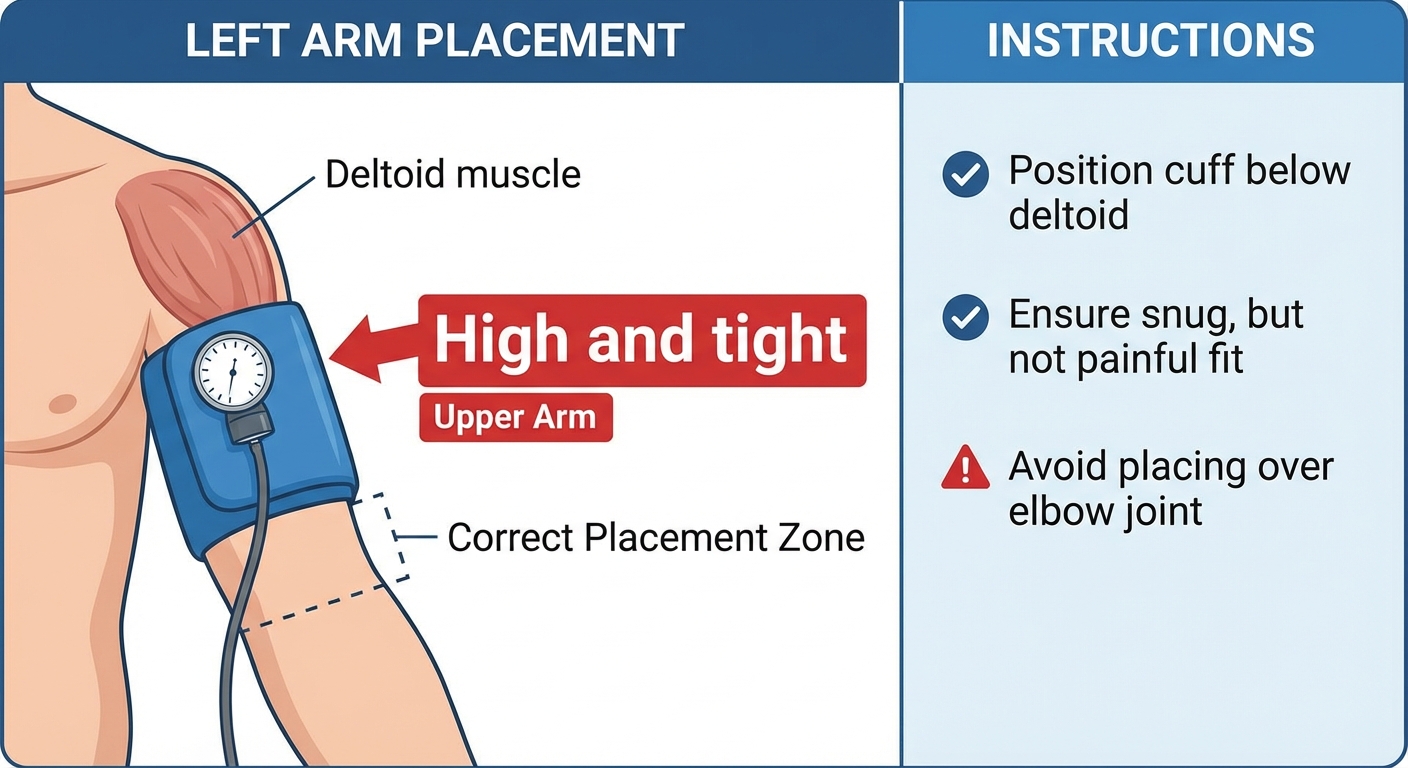
Pressure recommendations typically target 40-80% of complete arterial occlusion pressure. In practical terms, this means the cuff should feel tight, like a blood pressure cuff inflated partway, but you should still see color in your extremities and feel a pulse below the cuff. Dr. Loenneke’s research suggests that 40-50% occlusion provides the growth stimulus while minimizing risks, and that higher pressures don’t necessarily improve outcomes. For the upper body (smaller limbs, smaller vessels), pressures around 50% of occlusion work well. For the lower body (larger limbs, larger vessels), 60-80% may be needed to achieve similar restriction.
The training protocol itself follows a consistent pattern across the research. The standard approach uses 30 repetitions on the first set, followed by three sets of 15 repetitions, with 30-60 seconds rest between sets. Cuffs remain inflated throughout the entire sequence, including rest periods, which maintains the hypoxic and metabolic stress. Total time under restriction should not exceed 15-20 minutes per limb. The load is typically 20-30% of one-rep maximum, which feels almost embarrassingly light during the first few reps but becomes extremely challenging as metabolic stress accumulates.
Isolation exercises work most effectively for BFR because they allow complete restriction above the working muscle. Bicep curls, tricep extensions, leg extensions, leg curls, and calf raises are the most commonly used and researched movements. Compound movements like squats or presses can be performed with BFR but are more complex to execute properly and may not provide additional benefit over isolation work. Most practitioners reserve BFR for accessory movements rather than primary lifts.
Who Benefits Most: Rehabilitation and Beyond
While bodybuilders use BFR to squeeze out extra growth, its most profound application remains clinical. The ability to stimulate anabolism without high mechanical stress makes it transformative for populations who simply cannot lift heavy. For someone with osteoarthritis, a healing fracture, or recovering from joint surgery, the loads required for traditional strength training are often painful or contraindicated. BFR offers a workaround that changes rehabilitation outcomes.
Post-surgical patients represent the clearest application. After ACL reconstruction, for example, patients typically cannot perform heavy leg exercises for months. Yet quadriceps atrophy begins within days of surgery and predicts longer recovery times and poorer outcomes. Research from the Journal of Orthopaedic & Sports Physical Therapy demonstrates that incorporating BFR into post-ACL rehabilitation protocols significantly reduces muscle loss and accelerates strength recovery compared to standard protocols. Similar findings exist for knee replacement, hip surgery, and shoulder reconstruction.
Older adults face a different but related challenge. Sarcopenia, the age-related loss of muscle mass, accelerates after age 60 and contributes to falls, fractures, and loss of independence. Traditional strength training effectively combats sarcopenia, but many older adults have joint issues, osteoarthritis, or osteoporosis that make heavy lifting risky. BFR provides the muscle-building stimulus without the joint stress, making it an attractive option for this population. A 2018 study in Experimental Gerontology found that 12 weeks of BFR training improved muscle strength and mass in adults over 65 without adverse events.
Athletes use BFR differently, typically as supplementary training rather than primary work. During de-load weeks, when training volume is deliberately reduced, BFR can maintain muscle mass without the recovery burden of heavy lifting. Athletes returning from injury can begin resistance training earlier with BFR before progressing to traditional loads. Some endurance athletes incorporate BFR to build leg strength without the muscle mass gain that heavy squatting might produce. The versatility makes it a useful tool across multiple athletic contexts when applied thoughtfully.
Safety Considerations: Risks and Contraindications
Anytime you interfere with the vascular system, safety demands attention. The concept of restricting blood flow sounds inherently dangerous, and while BFR has a strong safety record when performed correctly, specific risks exist that must be respected. Understanding contraindications and warning signs prevents the adverse events that poor application can cause.
Absolute contraindications for BFR include blood clotting disorders, history of deep vein thrombosis (DVT), active varicose veins, peripheral vascular disease, uncontrolled hypertension, and pregnancy. The venous pooling that makes BFR effective also creates conditions that could trigger clotting events in susceptible individuals. Anyone with cardiovascular concerns should consult a physician before attempting BFR training. The risk-benefit calculation that favors BFR for rehabilitation patients doesn’t apply to individuals with vascular pathology.
Even for healthy individuals, proper execution matters. Too much pressure is more dangerous than too little. Complete arterial occlusion (no blood entering the limb) provides no additional benefit over partial restriction and dramatically increases risks including nerve damage and tissue hypoxia. The cuffs should never cause numbness, tingling, extreme pain, or color changes in the restricted limb. These symptoms indicate excessive pressure and require immediate cuff removal. Similarly, cuffs should not remain inflated for extended periods; the 15-20 minute maximum exists because longer restriction increases adverse event risk without improving outcomes.
Common execution errors include using cuffs that are too narrow (which concentrates pressure and increases nerve impingement risk), restricting multiple limbs simultaneously (which increases cardiovascular stress), poor cuff positioning (too distal placement fails to restrict the target muscles), and simply applying too much pressure in pursuit of more extreme results. Starting conservatively, with lower pressure and shorter duration, then progressing gradually as you understand your response to restriction, represents the safest approach. Working with a physical therapist or trainer experienced in BFR protocols provides valuable guidance during the learning phase.
The Bottom Line
Blood Flow Restriction training is a legitimate, research-supported method for building muscle with light loads. The mechanisms are well understood: metabolic stress, cell swelling, and early fast-twitch fiber recruitment combine to create growth signals that normally require heavy lifting. The research is extensive: hundreds of studies across diverse populations confirm efficacy for both muscle growth and strength development.
BFR doesn’t replace traditional strength training entirely. For maximum strength development and functional performance, heavy compound lifts remain superior. But BFR provides a valuable alternative when heavy lifting isn’t possible or practical, whether due to injury, joint issues, age-related limitations, or simply lack of equipment. For older adults navigating these challenges, our guide on strength training after 50 provides additional context on adapting resistance training to aging bodies. The ability to build significant muscle with 20-30% of maximum load represents a powerful option for people who thought strength training wasn’t available to them.
If you’re interested in trying BFR, invest in proper equipment with pressure gauges, learn the correct protocols, understand the contraindications, and start conservatively. The combination of light loads, short sessions, and substantial results makes BFR worth exploring, particularly for those navigating rehabilitation or seeking joint-friendly training options. BFR pairs well with other recovery-enhancing practices; cold water immersion can help manage inflammation between sessions while supporting the adaptation process.
Your BFR Starter Protocol:
- Acquire proper equipment: pneumatic cuffs with pressure gauges are safest
- Position cuffs high on limb (upper arm below shoulder, upper thigh below hip)
- Set pressure to 40-50% of occlusion (tight but with maintained pulse and color)
- Perform isolation exercises: 30 reps, then 3x15 reps, 30-60 second rest
- Use 20-30% of 1RM (feels light initially, very hard by final sets)
- Keep cuffs on for entire sequence but remove after 15-20 minutes maximum
- Start with 2x weekly per muscle group, monitor response before increasing
Sources: British Journal of Sports Medicine BFR meta-analysis (Grønfeldt 2019), Acta Physiologica BFR vs. traditional training comparison (Fahs 2012), Journal of Applied Physiology hormonal response studies, American Journal of Sports Medicine rehabilitation applications, Journal of Orthopaedic & Sports Physical Therapy ACL rehabilitation research, Sports Medicine strength gains systematic review (Hughes 2017), University of Mississippi BFR research (Dr. Jeremy Loenneke), Experimental Gerontology older adult BFR studies.





