Robert Waldinger has spent his career studying what makes people happy. As the fourth director of the Harvard Study of Adult Development, the longest-running study of adult life ever conducted, he inherited 85 years of data tracking the lives of 724 men from their teenage years into old age. The study expanded to include their wives, then their children, now spanning three generations. After analyzing decades of physical exams, blood tests, brain scans, and interviews, the research team arrived at a conclusion that surprised even them: the single strongest predictor of healthy aging wasn’t cholesterol levels, exercise habits, or even genetics. It was the quality of close relationships.
This finding isn’t an isolated curiosity from one longitudinal study. A 2023 meta-analysis published in Nature Human Behaviour, synthesizing data from 90 studies involving over 2.2 million participants, confirmed that social isolation and loneliness increase mortality risk by 26% and 29% respectively. To put this in perspective, smoking increases mortality risk by approximately 30%. The effect of loneliness on lifespan is comparable to smoking 15 cigarettes daily. Unlike smoking, however, loneliness carries no warning labels, and no public health campaigns target it with anything like the intensity applied to tobacco.
The implications extend far beyond individual health choices. We are experiencing what U.S. Surgeon General Vivek Murthy has called an “epidemic of loneliness,” with rates of social isolation roughly doubling since the 1980s. The average American in 2025 has fewer close friends, attends fewer community gatherings, and reports higher levels of chronic loneliness than at any point in measured history. Understanding the mechanisms by which social connection affects mortality, and the evidence-based interventions that can strengthen it, has become a public health priority with implications for both individual and societal wellbeing.
The Biology of Belonging: Why Isolation Kills
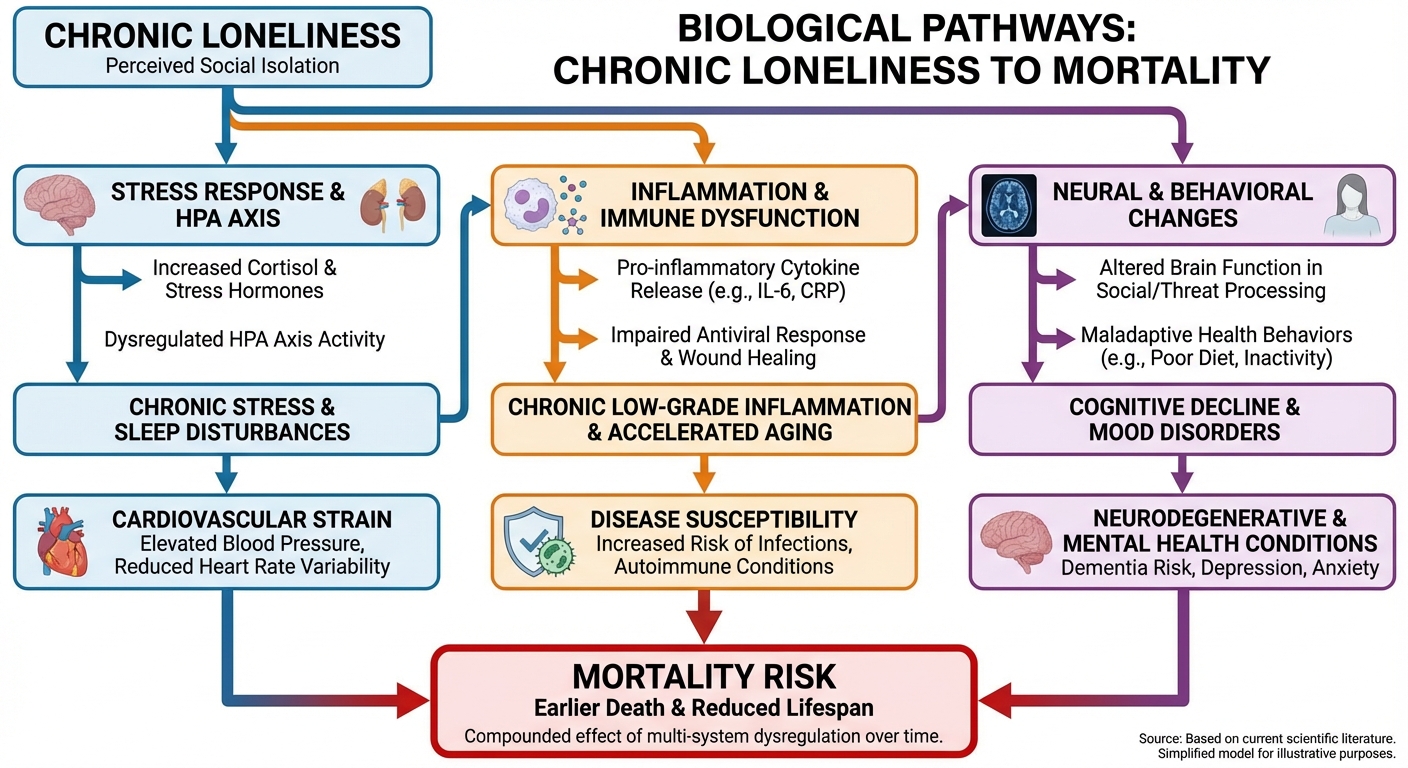
The relationship between social connection and mortality isn’t merely correlational; it operates through identified biological mechanisms that researchers have traced at the molecular level. Understanding these pathways reveals why social isolation is a physiological threat, not just a psychological discomfort.
Chronic loneliness activates the hypothalamic-pituitary-adrenal (HPA) axis, the body’s central stress response system. In ancestral environments, social isolation signaled genuine danger: humans separated from their groups faced predation, starvation, and environmental exposure. The brain evolved to treat isolation as a threat state requiring vigilance. This makes sense when isolation is temporary and the threat is real. But when loneliness becomes chronic, the sustained HPA activation produces persistently elevated cortisol that damages multiple organ systems over time.
Dr. Steve Cole at UCLA has pioneered research into the “conserved transcriptional response to adversity” (CTRA), a pattern of gene expression that shifts during chronic stress and isolation. Lonely individuals show upregulation of genes involved in inflammation and downregulation of genes involved in antiviral responses and antibody production. This pattern, which Cole’s team can identify from a simple blood draw, creates a pro-inflammatory state that accelerates cardiovascular disease, impairs wound healing, and compromises immune surveillance against cancer cells.
The cardiovascular effects are particularly well-documented. A 2016 meta-analysis in Heart found that loneliness and social isolation were associated with a 29% increased risk of coronary heart disease and a 32% increased risk of stroke. The mechanisms include the direct effects of chronic cortisol on blood vessel walls, increased inflammatory markers (CRP, IL-6) that drive atherosclerosis, and the health behaviors that often accompany isolation: poor sleep, reduced physical activity, and less motivation for preventive healthcare.
Quality Over Quantity: What Actually Matters in Relationships
The research on social connection and health reveals an important nuance: the number of social contacts matters far less than their quality. Having hundreds of social media followers while lacking a single person you could call in a crisis provides no protective health effect. The Harvard study and subsequent research consistently show that relationship depth, not breadth, predicts longevity.
Dr. Julianne Holt-Lunstad, whose meta-analyses have shaped our understanding of social connection and mortality, distinguishes between three related but distinct concepts. Social isolation refers to the objective lack of social contact, measurable by counting interactions. Loneliness is the subjective feeling of being alone, which can occur even among people with extensive social networks. Perceived social support describes whether someone believes help would be available if needed. All three independently predict mortality, but perceived social support shows the strongest effects.
This distinction explains why some highly social individuals die early while some relative loners live long, healthy lives. An extrovert with a packed social calendar but no confidants may be more physiologically stressed than an introvert with two deeply trusted friends. The protective factor isn’t activity but attachment: having people who know you deeply, accept you fundamentally, and would reliably help if you needed them.
Research from the University of North Carolina found that the number of social connections matters more in adolescence and old age, while relationship quality matters more in midlife. Young people benefit from broad social exposure that shapes identity development; older adults benefit from maintaining social engagement as peers and spouses die. But in the decades between, the quality of close relationships outweighs the quantity of casual ones. For a 45-year-old, having one deeply intimate relationship may be more protective than having twenty acquaintances.
The implications for how we invest our social energy are profound. Time spent maintaining shallow connections at the expense of deepening important ones may actually reduce the health benefits we receive from social life. The research supports what many intuitively sense: a few genuine friends outweigh many superficial ones.
Marriage, Family, and the Intimacy Gradient
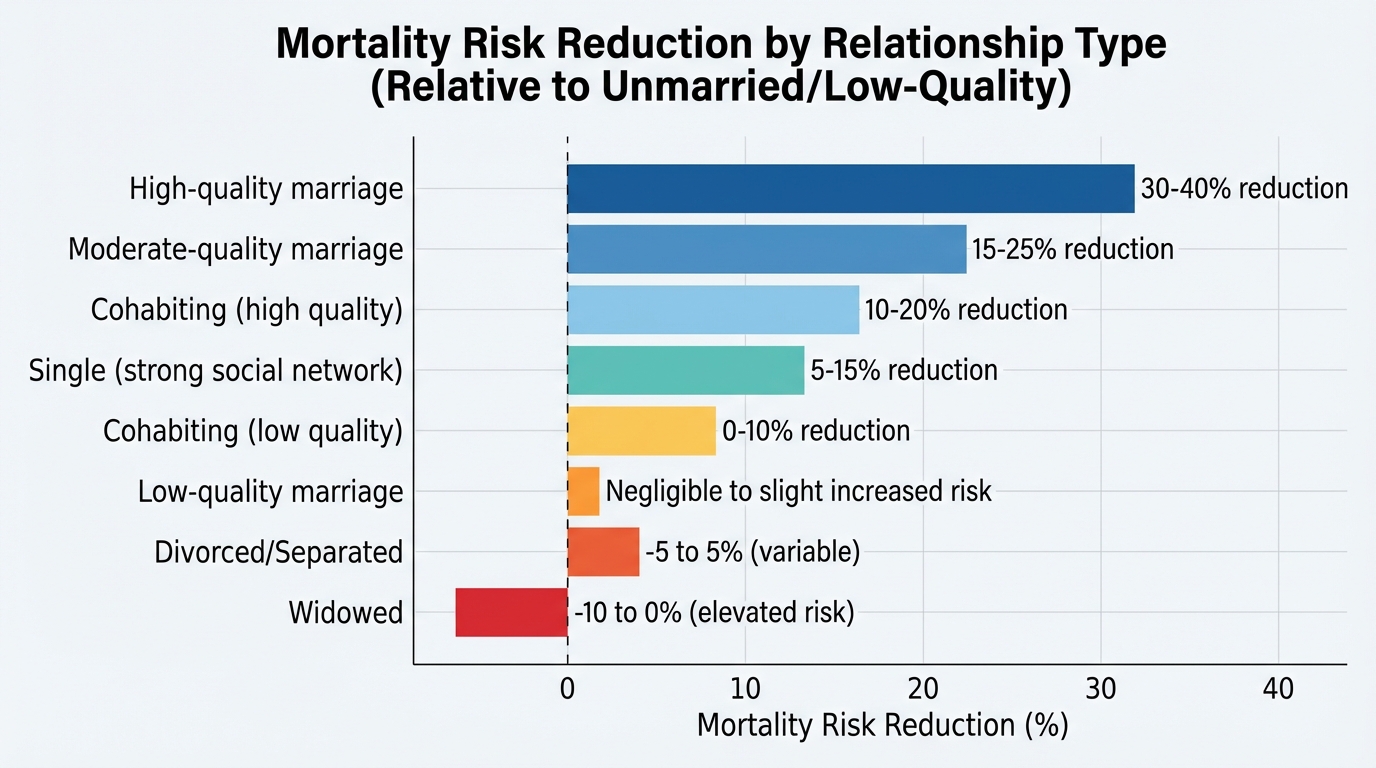
Among all social relationships, marriage and equivalent committed partnerships show the strongest associations with longevity. Married individuals live longer than unmarried individuals across nearly all studies, with the effect stronger for men than women. But the research reveals important complexities that simple “marriage is good for health” summaries obscure.
The health benefits of marriage depend entirely on marital quality. High-conflict marriages produce worse health outcomes than being single. The stress of chronic marital discord, with its attendant cortisol elevations, sleep disruption, and emotional exhaustion, eliminates and potentially reverses the protective effects of partnership. A longitudinal study published in Psychosomatic Medicine found that couples reporting high marital strain had worse health outcomes than divorced individuals. The lesson isn’t that marriage is inherently protective but that good relationships are protective and bad relationships are harmful.
The mechanisms behind marriage’s health effects extend beyond emotional support. Married individuals are more likely to receive encouragement for healthy behaviors: spouses remind each other about medications, discourage excessive drinking, and provide accountability for exercise and diet. They’re more likely to have health insurance and greater financial stability. They have someone who will notice when something seems wrong and encourage medical attention. These practical benefits compound over decades.
Family relationships beyond the marital dyad also contribute to longevity, though the effects are more complex. The Blue Zones research consistently finds that multi-generational households and strong family ties characterize long-lived populations. Singapore’s longevity policies explicitly encourage children to live near aging parents because this proximity correlates with reduced elder mortality. Grandparents who maintain active relationships with grandchildren show improved cognitive function and reduced depression compared to those without intergenerational contact.
However, family relationships can also be sources of chronic stress when characterized by conflict, obligation without genuine connection, or caregiving burden without adequate support. The health effects of family depend, like marriage, on quality rather than mere existence.
Friendship in Adulthood: The Overlooked Health Investment
While research attention focuses heavily on marriage and family, friendship represents an undervalued health asset that may be particularly important as family structures shift and geographic mobility increases. Unlike family relationships, friendships are entirely voluntary: they must be continuously chosen by both parties, creating a different psychological dynamic than bonds maintained by obligation or proximity.
Research from Michigan State University found that friendships become more important for health and happiness as people age, while family relationships remained relatively constant in their impact. Among older adults, having strong friendships was a better predictor of health than having strong family relationships. The researchers hypothesized that friendships, because they’re voluntary, are more responsive to incompatibility: bad friendships end, while bad family relationships often continue due to obligation. The friendships that survive decades are likely to be genuinely supportive.
The challenge is that adult friendships are difficult to form and maintain. After leaving the structured environments of school and early career, opportunities for the repeated, unplanned interactions that generate friendship decline dramatically. Making friends in midlife requires intentional effort that the time pressures of career and family make difficult. One survey found that the average American hasn’t made a new close friend in five years.
The investment required to maintain friendships is substantial but quantifiable. Research suggests that close friendships require roughly 200 hours of shared time to develop and ongoing contact of at least weekly frequency to maintain. In a life already compressed by work, family obligations, and personal maintenance, finding these hours requires treating friendship as a genuine priority rather than something that happens if time permits.
Practical strategies for adult friendship formation include joining structured groups with repeated contact (sports leagues, book clubs, volunteer organizations), converting acquaintances to friends through one-on-one invitations, and using technology to maintain geographically distant connections through regular video calls rather than passive social media interaction.
Community and Purpose: Beyond Individual Relationships
The health effects of social connection extend beyond dyadic relationships to include community belonging and sense of purpose. Participation in religious communities, civic organizations, volunteer groups, and other collective structures provides mortality benefits independent of the close relationships that may form within them.
The mechanisms appear to involve both social and psychological factors. Community participation provides regular social contact, shared rituals that create meaning, and roles that contribute to identity beyond family and work. Religious attendance, one of the most studied forms of community participation, is associated with approximately 30% reduced mortality in some studies, an effect that remains significant after controlling for health behaviors and social support from individual relationships.
Dr. Richard Sloan at Columbia has cautioned against interpreting these findings as evidence that religion itself is healthy, noting that religious attendance is confounded with numerous other factors including socioeconomic status, social networks, and health behaviors. Nonetheless, the consistent finding across studies suggests that community belonging, whatever its specific form, provides something that individual relationships alone don’t fully replace.
Volunteering shows particularly strong associations with health and longevity, especially among older adults. A 2020 meta-analysis found that volunteers had 22% lower mortality than non-volunteers. The effects may operate through multiple pathways: the physical activity involved in many volunteer roles, the social connections formed, the sense of purpose and meaning derived from helping others, and the cognitive stimulation of learning new skills. For those seeking to improve health through social connection, volunteering offers a reliable way to simultaneously expand social networks and contribute to something beyond oneself.
Building Connection: Evidence-Based Intervention Strategies
Understanding that social connection affects mortality creates an obvious question: what can individuals actually do to strengthen their social ties? The research points toward specific, actionable strategies with documented effectiveness.
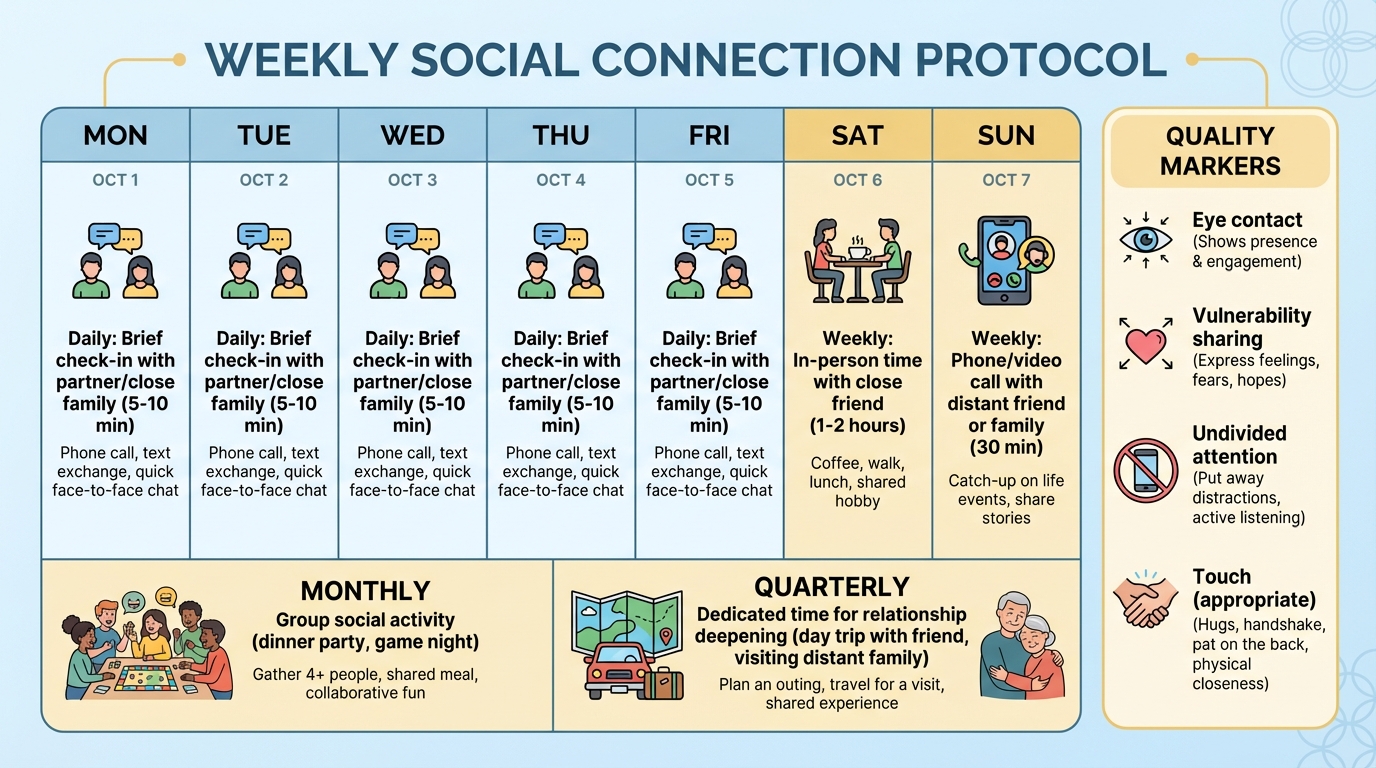
Prioritize in-person contact over digital communication. While video calls maintain connections across distances, text-based communication and social media provide weaker physiological benefits. The stress-buffering effects of social support are strongest during face-to-face interaction, where touch, eye contact, and vocal tone activate the parasympathetic nervous system and reduce cortisol. Technology should supplement rather than replace in-person contact wherever possible.
Schedule social time with the same priority as work and exercise. Treating social connection as something that happens with leftover time guarantees it won’t happen. Research on habit formation suggests that consistent weekly commitments (a standing dinner with friends, a regular phone call with a parent) are more sustainable than sporadic intense socializing. The Brigham Young mortality research found that consistent moderate social contact was more protective than inconsistent intensive contact.
Deepen existing relationships before pursuing new ones. Given that relationship quality matters more than quantity, investing in the relationships you already have may yield greater health returns than expanding your network. This means moving beyond surface-level interaction: sharing vulnerabilities, asking deeper questions, and spending time in activities that allow real conversation rather than parallel attention to screens or spectacles.
Address loneliness as a health problem, not a character flaw. The stigma around admitting loneliness prevents many people from taking action. Reframing loneliness as a signal, like hunger or pain, that indicates a genuine need rather than a personal failing may reduce the shame that keeps people isolated. If you’re lonely, you’re experiencing a health risk factor that warrants intervention as much as high blood pressure or elevated cholesterol.
For those experiencing chronic loneliness, professional support may be valuable. Cognitive-behavioral approaches can address the negative thought patterns that sometimes perpetuate isolation by making social interaction feel threatening. The gratitude practices that build psychological resilience can also help create the emotional foundation for reaching out to others.
The Bottom Line
Social connection isn’t a luxury or a personality preference; it’s a biological necessity with mortality effects rivaling traditional health behaviors. The 26% increased mortality risk from social isolation is comparable to smoking and exceeds the effects of obesity or physical inactivity. Yet while we have surgeon general warnings on cigarettes and widespread campaigns promoting exercise, social connection remains largely unaddressed as a public health priority.
The research is clear on several key points. Quality matters more than quantity: a few deep relationships outweigh many shallow ones. Marriage and family relationships are protective when high-quality but harmful when characterized by chronic conflict. Friendships become increasingly important for health as people age. Community participation and sense of purpose provide benefits beyond individual relationships.
Building and maintaining social connection requires intentional investment in a world that increasingly provides substitutes (social media, streaming entertainment) rather than genuine connection. Treating social time as a health behavior, scheduling it with the same priority as exercise or sleep, and deepening existing relationships rather than constantly seeking new ones offers the most practical path forward.
The Harvard Study of Adult Development, now entering its ninth decade, continues to follow its participants and their descendants. The message remains consistent: the people who aged best weren’t the richest, the most successful, or even the healthiest in midlife. They were the ones who invested in relationships. In the final accounting, Waldinger notes, “Good relationships keep us happier and healthier. Period.”
Action Steps:
- Audit your current social connections: identify your three closest relationships and assess their quality
- Schedule one recurring weekly social commitment with a friend or family member
- Convert one digital-only relationship to regular video calls or in-person contact
- Join one community group (volunteer organization, sports league, religious community, or interest-based club) for regular face-to-face interaction
- Practice vulnerability in one conversation this week: share something real rather than staying surface-level
Sources: Harvard Study of Adult Development (Dr. Robert Waldinger), Nature Human Behaviour meta-analysis on social isolation and mortality (2023), Brigham Young University social connection research (Dr. Julianne Holt-Lunstad), UCLA gene expression research (Dr. Steve Cole), Heart journal cardiovascular meta-analysis (2016), U.S. Surgeon General loneliness advisory (Dr. Vivek Murthy), Michigan State University friendship and aging research.