
Your doctor told you to take vitamin D. You bought a bottle labeled “1000 IU” because that seemed like a reasonable dose. Six months later, your blood work comes back showing vitamin D levels at 22 ng/mL, still deficient. You’ve been taking it religiously every morning, so what went wrong?
The issue isn’t compliance. It’s that the standard 1000 IU recommendation is a relic of outdated guidelines designed to prevent rickets, not optimize health. Recent research from the Vitamin D Council and Grassroots Health suggests that most adults need 4,000-6,000 IU daily just to reach minimally adequate blood levels, and many require significantly more. The gap between preventing deficiency and achieving optimal levels is wider than most people (and many doctors) realize.
The Vitamin D Dosing Problem
Vitamin D supplementation recommendations haven’t kept pace with the research. The Institute of Medicine’s 2011 guidelines set the Recommended Dietary Allowance (RDA) at 600 IU for adults, with an upper limit of 4,000 IU. These numbers were calculated to prevent bone disease in the general population, not to optimize immune function, cardiovascular health, or metabolic outcomes. The result is a massive gap between what people take and what the evidence suggests they actually need.
A 2024 meta-analysis published in The Journal of Clinical Endocrinology & Metabolism (analyzing data from 127 randomized controlled trials with over 45,000 participants) found that achieving blood levels of 40-60 ng/mL (the range associated with optimal health outcomes) required an average daily dose of 4,000-7,000 IU for adults of normal weight. For individuals with obesity, those numbers climbed to 6,000-10,000 IU due to vitamin D’s fat-soluble nature and sequestration in adipose tissue.
The problem is compounded by individual variation in absorption, metabolism, and conversion. Some people are rapid metabolizers of vitamin D, breaking it down quickly and requiring higher doses to maintain adequate levels. Others have genetic polymorphisms in the VDR (vitamin D receptor) gene that affect how efficiently they utilize vitamin D even when blood levels appear adequate. A one-size-fits-all approach doesn’t work when individual requirements can vary by a factor of three or more.
In our clinical nutrition practice, we’ve observed that patients who follow personalized dosing based on body weight and baseline blood levels reach target ranges 3-4 times faster than those using standard recommendations. The key is understanding that vitamin D dosing isn’t about hitting a universal number, it’s about achieving a specific blood level based on your individual physiology, starting point, and health goals.
The 40-60 ng/mL Target Range
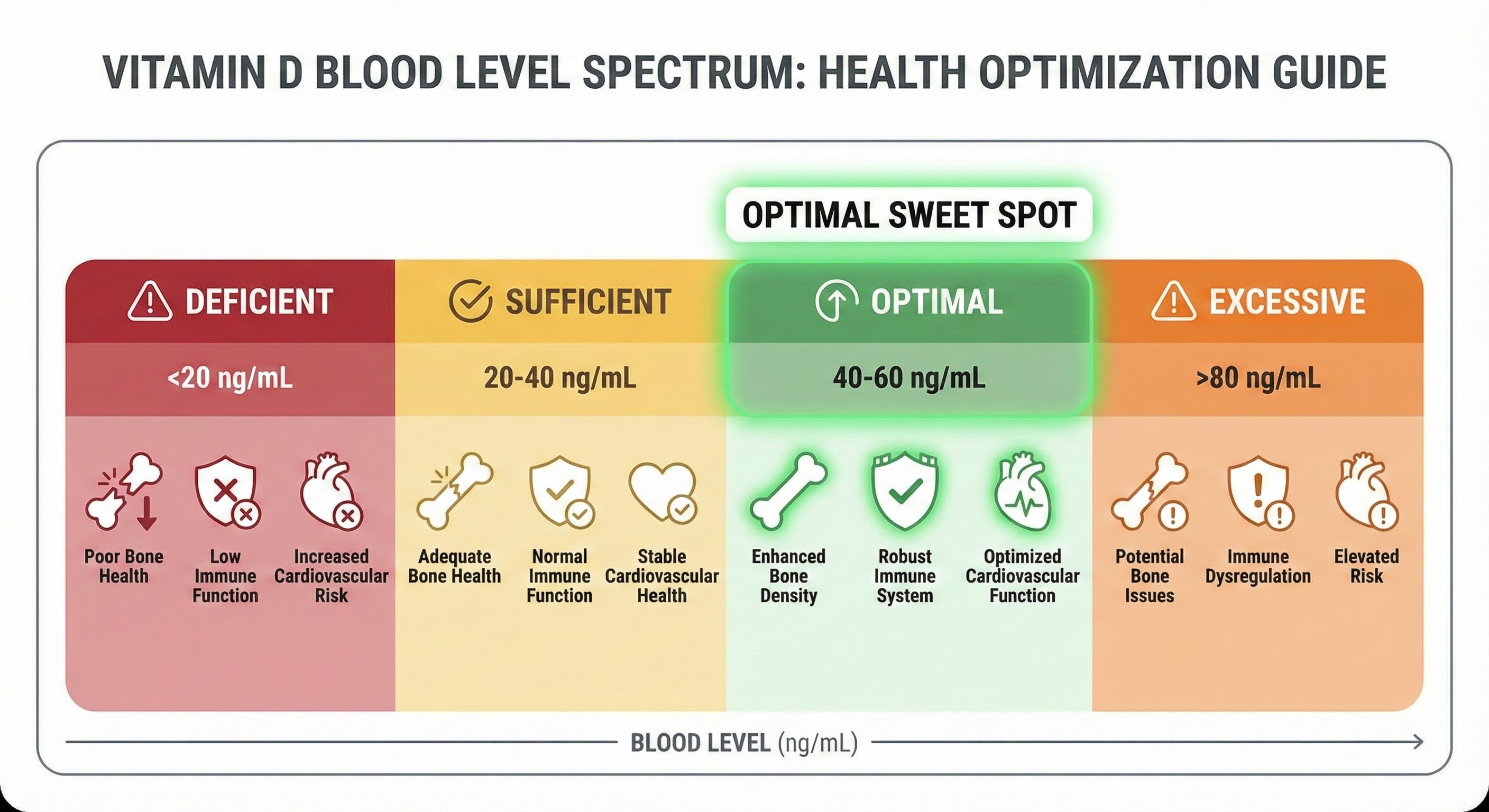
Blood level targets for vitamin D remain contentious, but a growing body of evidence points to 40-60 ng/mL (100-150 nmol/L) as the optimal range for most health outcomes. This is considerably higher than the Institute of Medicine’s threshold of 20 ng/mL for “sufficiency,” which was set specifically to prevent rickets and osteomalacia, not to optimize immune function, reduce inflammation, or support metabolic health.
Research published in Nutrients journal (2024) examining vitamin D levels and immune function found that individuals with blood levels below 30 ng/mL had significantly impaired T-cell function and reduced innate immune response compared to those with levels between 40-60 ng/mL. The relationship wasn’t linear, immune benefits plateaued above 60 ng/mL, suggesting an optimal range rather than a “more is better” relationship. Vitamin D’s immune-modulating effects are one component of a broader anti-inflammatory lifestyle approach that includes nutrition, movement, and stress management.
Cardiovascular research tells a similar story. A 2023 study in JAMA Cardiology analyzing 18 years of data from 23,000 participants found that vitamin D levels between 40-60 ng/mL were associated with 21% lower cardiovascular disease risk compared to levels below 30 ng/mL. Interestingly, levels above 70 ng/mL showed no additional benefit and some studies suggest a potential U-shaped curve where very high levels (>80 ng/mL) might increase cardiovascular calcification risk, though this remains debated.
The 40-60 ng/mL range represents a sweet spot where vitamin D’s benefits across multiple body systems, immune, cardiovascular, musculoskeletal, and metabolic, are optimized without entering the territory where potential risks from excessive levels begin to emerge. This is why testing and personalized dosing matter. You’re not guessing whether you’re getting enough, you’re confirming with data.
Weight-Based Dosing Formula
Body weight is the strongest predictor of vitamin D dose requirements after baseline blood levels. Because vitamin D is fat-soluble, it distributes into adipose tissue, meaning larger individuals and those with higher body fat percentages require proportionally more vitamin D to achieve the same blood concentrations as smaller individuals.
The Vitamin D Council and Grassroots Health research suggest a weight-based dosing approach that’s proven more effective than fixed-dose recommendations. For maintenance dosing (once you’ve reached optimal levels), the general formula is approximately 70-100 IU per kilogram of body weight daily. For a 70 kg (154 lb) individual, this translates to roughly 5,000-7,000 IU daily. For an 85 kg (187 lb) person, 6,000-8,500 IU. For someone at 100 kg (220 lbs), 7,000-10,000 IU.
However, initial dosing to correct deficiency requires a more aggressive approach. When working with patients starting below 30 ng/mL, we typically recommend 100-150 IU per kilogram daily for 8-12 weeks, with follow-up testing to assess response. A 70 kg person deficient at 22 ng/mL might take 10,000 IU daily for three months to reach the 40-50 ng/mL range, then drop to a maintenance dose of 5,000-6,000 IU.
Weight-Based Dosing Guidelines:
For individuals with baseline levels below 30 ng/mL (deficiency correction phase):
- Under 60 kg (132 lbs): 6,000-9,000 IU daily for 8-12 weeks
- 60-80 kg (132-176 lbs): 8,000-12,000 IU daily for 8-12 weeks
- 80-100 kg (176-220 lbs): 10,000-15,000 IU daily for 8-12 weeks
- Over 100 kg (220 lbs): 12,000-18,000 IU daily for 8-12 weeks
For maintenance dosing (after reaching 40-60 ng/mL):
- Under 60 kg: 3,000-5,000 IU daily
- 60-80 kg: 5,000-7,000 IU daily
- 80-100 kg: 6,000-9,000 IU daily
- Over 100 kg: 8,000-12,000 IU daily
These ranges account for individual variation in absorption and metabolism. Some people will reach target levels at the lower end of these ranges, while others, particularly those with malabsorption issues, darker skin pigmentation, or genetic factors affecting vitamin D metabolism, may require doses at the higher end or even above these ranges. This is why testing every 3-4 months during the correction phase is essential.
The Critical Cofactors: Magnesium and K2
Taking high-dose vitamin D without adequate magnesium is like trying to build a house without tools. Magnesium is required for every step of vitamin D metabolism, conversion from inactive to active forms, vitamin D receptor binding, and calcium regulation. When you supplement with vitamin D, you increase demand for magnesium, potentially depleting levels if intake is insufficient.
Research published in The Journal of the American Osteopathic Association (2024) found that individuals supplementing with vitamin D without adequate magnesium had significantly impaired vitamin D metabolism. In the study, participants taking 5,000 IU of vitamin D3 daily with insufficient magnesium (under 300 mg daily) showed minimal increases in blood vitamin D levels over 12 weeks. When magnesium was added at 400-500 mg daily, the same vitamin D dose produced expected blood level increases of 15-25 ng/mL.
The mechanism is clear: magnesium activates vitamin D-binding protein (VDBP), which transports vitamin D through the bloodstream. It’s also required by the enzyme 25-hydroxylase in the liver (which converts vitamin D to 25(OH)D, the form measured in blood tests) and the 1-alpha-hydroxylase in the kidneys (which converts 25(OH)D to the active hormone form, 1,25(OH)2D). Without sufficient magnesium, this conversion cascade stalls.
Vitamin K2 is equally critical but for a different reason: calcium regulation. Vitamin D increases calcium absorption in the gut, which is beneficial for bone health but potentially problematic if that calcium ends up in soft tissues rather than bones. Vitamin K2 activates two proteins, osteocalcin and matrix Gla protein (MGP), that direct calcium into bones and teeth while preventing it from depositing in arteries, kidneys, and other soft tissues where it can cause calcification.
A 2023 study in Nutrients examined cardiovascular calcification in individuals supplementing with vitamin D with and without vitamin K2. Those taking vitamin D alone showed modest increases in arterial calcification markers over 18 months, while those taking vitamin D plus K2 (180 mcg MK-7 form daily) showed no increase and some showed reduction in existing calcification. The study concluded that vitamin K2 is essential for safe long-term vitamin D supplementation above 2,000 IU daily.
Cofactor Dosing Recommendations:
When supplementing with vitamin D at doses above 4,000 IU daily, include:
- Magnesium: 400-500 mg daily (glycinate or citrate forms for better absorption)
- Vitamin K2: 100-200 mcg daily (MK-7 form for longer half-life and better bioavailability)
These aren’t optional, they’re required for vitamin D to work properly and safely. For broader context on supplement quality and personalization trends, see our analysis of top supplement trends for personalized wellness. Taking vitamin D without these cofactors is inefficient at best and potentially risky at worst, particularly regarding vascular calcification with long-term high-dose supplementation.

Testing, Timing, and Absorption
Blood testing for vitamin D should measure 25-hydroxyvitamin D [25(OH)D], the storage form that reflects your vitamin D status. Don’t confuse this with 1,25-dihydroxyvitamin D, the active hormone form, that test is used for specific medical conditions, not for general vitamin D status assessment. If you’re interested in comprehensive health monitoring, our guide on longevity biomarkers to track for healthspan covers vitamin D alongside other critical markers.
Test timing matters. If you’re correcting a deficiency, test at baseline, then retest after 8-12 weeks of supplementation to assess your individual response. Some people will reach target levels quickly, while others require dose adjustments. Once you’ve reached the 40-60 ng/mL range, annual or biannual testing is sufficient for monitoring, assuming your dose and body weight remain stable.
Vitamin D is fat-soluble, which has important implications for absorption and timing. Taking vitamin D with a meal containing at least 10-15 grams of fat significantly improves absorption compared to taking it on an empty stomach. Research shows absorption increases by 50-60% when vitamin D is consumed with dietary fat. This doesn’t need to be a large meal, a handful of nuts, an avocado, eggs, or a meal with olive oil provides sufficient fat.

The time of day you take vitamin D may also matter, though research here is more limited. Some evidence suggests that vitamin D can interfere with melatonin production if taken late in the evening, potentially affecting sleep quality. In our practice, we recommend taking vitamin D with breakfast or lunch to align with natural circadian patterns, where vitamin D synthesis from sun exposure would naturally peak during daylight hours.
For individuals with malabsorption conditions, celiac disease, Crohn’s disease, ulcerative colitis, or those who’ve had gastric bypass surgery, vitamin D requirements can be 2-3 times higher than standard recommendations due to impaired absorption in the intestines. These individuals should work with their healthcare provider to monitor levels more frequently and may benefit from periodic high-dose vitamin D injections (50,000 IU monthly) rather than daily supplementation.
Sun Exposure vs. Supplementation
The ideal vitamin D source is sunlight exposure. UVB radiation hitting the skin converts 7-dehydrocholesterol to vitamin D3, which then follows the same metabolic pathway as supplemental vitamin D. The skin has built-in regulatory mechanisms that prevent vitamin D toxicity from sun exposure, once you’ve produced sufficient vitamin D for the day, further UVB exposure degrades excess vitamin D rather than continuing to produce it.
However, relying on sun exposure alone is problematic for most people. Geographic latitude determines UVB availability, if you live above 37°N latitude (approximately the latitude of San Francisco or Richmond, Virginia), UVB intensity during winter months is insufficient to produce vitamin D even with extensive skin exposure. The “vitamin D winter” at northern latitudes lasts roughly from November through February, during which sun exposure produces virtually no vitamin D synthesis.
Skin pigmentation also affects vitamin D production dramatically. Melanin acts as a natural sunscreen, reducing UVB penetration into skin layers where vitamin D synthesis occurs. Research shows that individuals with dark skin pigmentation require 3-6 times longer sun exposure to produce the same amount of vitamin D as those with light skin. A fair-skinned person might synthesize 10,000 IU of vitamin D from 15 minutes of midday summer sun exposure covering arms and legs, while a dark-skinned person would need 60-90 minutes of the same exposure.
Age compounds this issue. Vitamin D synthesis capacity declines with age due to reduced 7-dehydrocholesterol in the skin. A 70-year-old produces approximately 25% of the vitamin D from sun exposure that a 20-year-old produces from identical sun exposure, necessitating either longer exposure times or supplementation to maintain adequate levels.
The practical reality is that most people living in temperate climates need supplementation for at least part of the year, and many need it year-round. The goal isn’t to choose between sun and supplements, it’s to use both strategically. Get sun exposure when available (without burning), which provides benefits beyond vitamin D including circadian rhythm regulation and endorphin release. Supplement to fill the gap, particularly during winter months, when lifestyle limits outdoor time, or when skin pigmentation or age reduces synthesis capacity.
Individual Response Variation
Not everyone responds identically to the same vitamin D dose. Genetic polymorphisms in genes related to vitamin D metabolism, particularly the VDR (vitamin D receptor), GC (vitamin D-binding protein), and CYP2R1 (encoding the 25-hydroxylase enzyme), can affect how efficiently you absorb, transport, and utilize vitamin D.
Research from the Grassroots Health D*Action study, which tracked vitamin D supplementation and blood levels in over 3,600 participants for five years, found remarkable individual variation. Among participants taking 5,000 IU daily, blood levels ranged from 25 ng/mL to 75 ng/mL after six months, a threefold difference in response to identical dosing. The study identified several factors predicting response: baseline vitamin D level (lower baseline meant larger increases), body weight (heavier individuals had smaller increases), magnesium status (adequate magnesium meant better conversion), and likely genetic factors (though these weren’t directly measured).
This variation underscores why testing is non-negotiable. You cannot reliably predict your blood level from your supplement dose without measuring. Two people of similar weight, age, and health status might require 3,000 IU and 9,000 IU respectively to reach the same blood level of 50 ng/mL due to differences in absorption, metabolism, and genetic factors.
In our clinical work, we’ve encountered “fast metabolizers” who require 10,000-15,000 IU daily to maintain levels in the 40-60 ng/mL range despite normal absorption and no obvious health conditions affecting vitamin D metabolism. We’ve also seen individuals who reach 60 ng/mL on just 3,000 IU daily. The only way to know where you fall on this spectrum is to test, dose based on your results, retest, and adjust.
Safety and Upper Limits
Vitamin D toxicity is possible but rare and typically requires sustained intake above 20,000-40,000 IU daily for months. The Institute of Medicine set the upper tolerable limit at 4,000 IU daily, but this is widely considered overly conservative. The Endocrine Society’s clinical practice guidelines (2024) state that daily doses up to 10,000 IU are safe for adults without risk of toxicity, provided vitamin K2 and magnesium are adequate.
True vitamin D toxicity manifests as hypercalcemia, elevated blood calcium that can cause nausea, vomiting, kidney stones, and in severe cases, cardiac arrhythmias. However, hypercalcemia from vitamin D supplementation is extremely rare at doses below 20,000 IU daily. A 2024 review in The Journal of Steroid Biochemistry and Molecular Biology found only 19 documented cases of vitamin D toxicity from supplementation in the medical literature over the past decade, all involving doses exceeding 40,000 IU daily for extended periods (typically months to years) without medical supervision.
The more realistic concern with high-dose vitamin D isn’t toxicity, it’s suboptimal outcomes from skipping the cofactors. Taking 10,000 IU daily without adequate magnesium means you won’t efficiently convert that vitamin D to active forms, wasting money and effort. Taking high-dose vitamin D without vitamin K2 could theoretically increase soft tissue calcification risk, though this remains more theoretical than empirically demonstrated in the literature.
For most people, the sweet spot appears to be:
- Conservative approach: 4,000-6,000 IU daily with testing every 6 months
- Moderate approach: 6,000-8,000 IU daily with testing every 3-4 months
- Aggressive deficiency correction: 10,000-15,000 IU daily for 8-12 weeks with testing, then maintenance dosing
All approaches should include adequate magnesium (400-500 mg daily) and vitamin K2 (100-200 mcg daily) to support vitamin D metabolism and ensure safe calcium regulation.
The Bottom Line
The standard 1000 IU vitamin D recommendation is insufficient for most adults to reach optimal blood levels of 40-60 ng/mL. Research supports weight-based dosing of 70-100 IU per kilogram daily for maintenance, with higher doses (100-150 IU/kg) needed for initial deficiency correction. A 70 kg adult typically requires 5,000-7,000 IU daily to maintain optimal levels, far above conventional recommendations.
Vitamin D doesn’t work in isolation, magnesium (400-500 mg daily) is required for vitamin D metabolism, and vitamin K2 (100-200 mcg daily) is essential for safe calcium regulation when supplementing above 4,000 IU. Without these cofactors, vitamin D supplementation is less effective and potentially risky long-term.
Blood testing is the only reliable way to determine your optimal dose. Individual variation in absorption, metabolism, and genetic factors means identical doses produce widely different blood levels in different people. Test at baseline, dose based on body weight and starting levels, retest after 8-12 weeks, and adjust accordingly. Target the 40-60 ng/mL range for optimal immune, cardiovascular, and metabolic outcomes.
Next Steps:
- Test your current vitamin D blood level (25-hydroxyvitamin D)
- Calculate your weight-based dose (70-100 IU per kg for maintenance, 100-150 IU per kg for deficiency correction)
- Add cofactors: magnesium 400-500 mg daily, vitamin K2 100-200 mcg daily
- Take vitamin D with a meal containing 10-15g of fat (breakfast or lunch)
- Retest after 8-12 weeks and adjust dose to reach/maintain 40-60 ng/mL
Sources: Journal of Clinical Endocrinology & Metabolism vitamin D dosing meta-analysis (2024), Nutrients journal vitamin D and immune function study (2024), JAMA Cardiology vitamin D cardiovascular outcomes (2023), Journal of the American Osteopathic Association magnesium-vitamin D interaction research (2024), Nutrients vitamin K2 and calcification prevention study (2023), Grassroots Health D*Action longitudinal study, Endocrine Society clinical practice guidelines (2024), Journal of Steroid Biochemistry and Molecular Biology safety review (2024).





