
Stroke kills roughly 162,000 Americans each year and is the fourth leading cause of death among women in the United States. For women over 55, the risk climbs steeply as estrogen levels decline during and after menopause, stripping away a hormone that normally protects blood vessels, reduces inflammation, and supports healthy blood flow to the brain. The numbers are bleak, but a new study tracking more than 105,000 women over two decades offers concrete evidence that what you put on your plate can meaningfully shift the odds in your favor.
Researchers from the City of Hope Comprehensive Cancer Center, Charles R. Drew University, and Columbia University published their findings in Neurology Open Access on February 4, 2026, reporting that women who closely followed the Mediterranean diet were 18% less likely to have any type of stroke. The protection was even stronger for hemorrhagic stroke, the deadlier subtype caused by bleeding in the brain, where high-adherence women saw a 25% risk reduction. The study drew on the California Teachers Study, one of the largest and longest-running prospective cohort studies of women in the country, and its 21-year follow-up period makes it one of the most durable investigations of diet and stroke risk ever conducted.
Inside the 105,000-Woman California Teachers Study
The California Teachers Study began in 1995 when researchers enrolled 133,477 female educators and school administrators who were members of the California State Teachers’ Retirement System. For this stroke analysis, the team narrowed the cohort to 105,614 women with no prior history of stroke, all with an average age of 53 at baseline. Participants completed detailed food frequency questionnaires covering their eating habits and portion sizes over the previous year. Researchers then scored each woman’s dietary adherence using a validated 9-point Mediterranean diet scale that has become a standard tool in nutritional epidemiology.
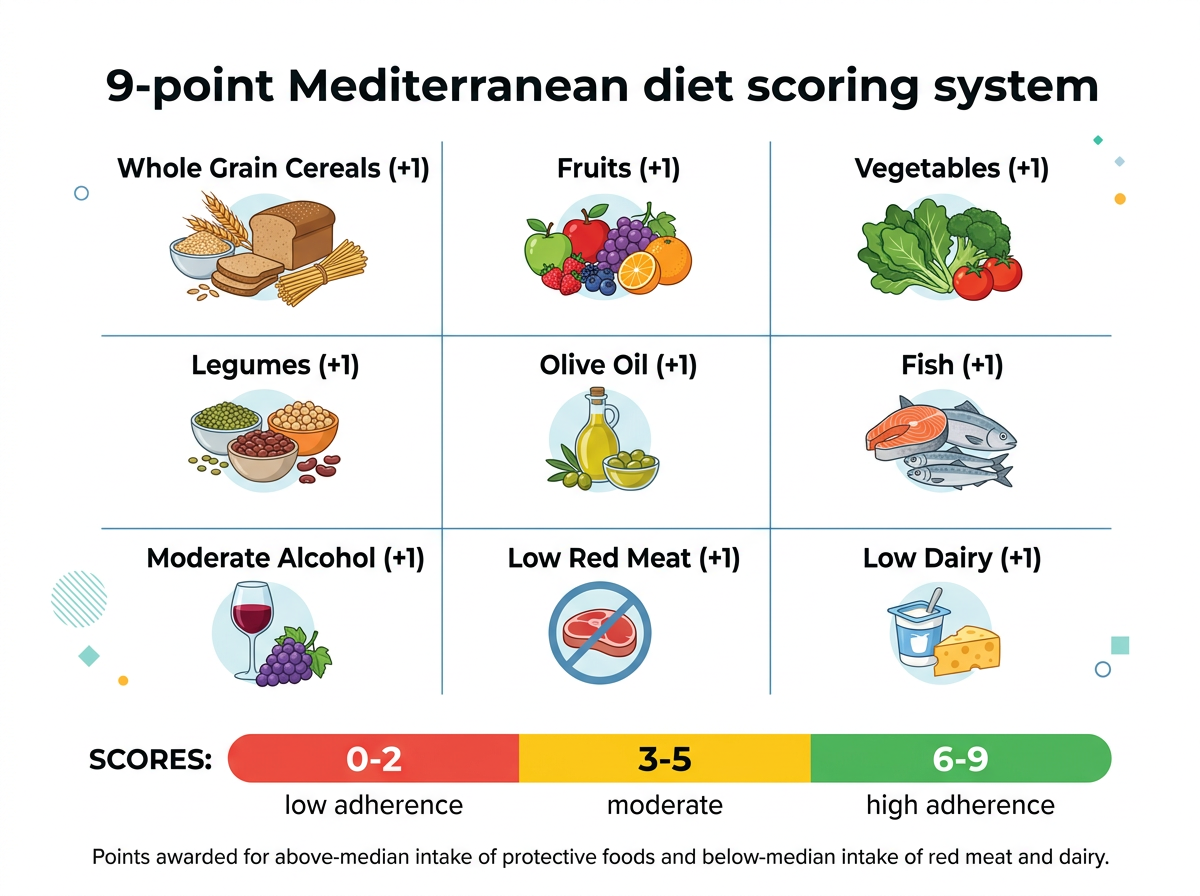
The scoring system awarded one point for consuming above the population median in each of seven food categories: whole grain cereals, fruits, vegetables, legumes, olive oil, fish, and moderate alcohol. Participants also earned one point each for consuming below the median in two categories: red meat and dairy products. Scores ranged from 0 (no adherence) to 9 (highest adherence). Approximately 30% of the women scored between 6 and 9, placing them in the highest adherence group, while 13% scored between 0 and 2, the lowest group.
Over a mean follow-up of 20.5 years (through 2020), researchers documented 4,083 strokes: 3,358 ischemic strokes (caused by blood clots blocking brain arteries) and 725 hemorrhagic strokes (caused by bleeding within the brain). After adjusting for confounding variables including smoking status, physical activity, and hypertension, the results were clear. Women in the highest adherence group had an 18% lower risk of any stroke, a 16% lower risk of ischemic stroke, and a 25% lower risk of hemorrhagic stroke compared to women in the lowest adherence group.
“Our findings support the mounting evidence that a healthy diet is critical to stroke prevention,” said Sophia S. Wang, PhD, molecular epidemiologist at the City of Hope Comprehensive Cancer Center and lead author of the study. She added a note about the hemorrhagic findings specifically: “We were especially interested to see that this finding applies to hemorrhagic stroke, as few large studies have looked at this type of stroke.” That distinction matters because hemorrhagic strokes, while less common than ischemic strokes, carry a significantly higher mortality rate and have received far less attention in dietary research.
Why the Mediterranean Diet Protects Blood Vessels
The Mediterranean dietary pattern reduces stroke risk through several overlapping biological mechanisms, and understanding these pathways explains why the protection is so consistent across different study designs, populations, and follow-up periods. The primary mechanism is anti-inflammatory action. Chronic, low-grade inflammation damages the endothelial lining of blood vessels over time, promoting atherosclerosis (plaque buildup in arteries) and increasing the likelihood that plaques will rupture and form clots. The Mediterranean diet’s emphasis on polyphenol-rich foods, omega-3 fatty acids, and monounsaturated fats directly counteracts this inflammatory cascade.
Extra-virgin olive oil, the diet’s primary fat source, contains polyphenolic compounds including hydroxytyrosol, oleuropein, and oleocanthal that reduce levels of C-reactive protein (CRP) and interleukin-6 (IL-6), two of the most reliable blood markers of systemic inflammation. Oleocanthal in particular has demonstrated anti-inflammatory potency comparable to low-dose ibuprofen in laboratory studies. Olive oil also enhances endothelial function by increasing nitric oxide availability, which relaxes blood vessels and improves blood flow. The landmark PREDIMED trial, published in The New England Journal of Medicine, found that a Mediterranean diet supplemented with extra-virgin olive oil reduced cardiovascular events (including stroke) by 30% compared to a low-fat control diet.
Omega-3 fatty acids from fish, another cornerstone of the diet, reduce triglycerides, lower blood pressure, decrease platelet aggregation (clumping that triggers clots), and shift immune cells toward an anti-inflammatory state. These effects are particularly relevant for ischemic stroke prevention. Meanwhile, the diet’s high fiber content from whole grains, legumes, fruits, and vegetables promotes the production of short-chain fatty acids in the gut, which have systemic anti-inflammatory effects that benefit vascular health throughout the body. Magnesium, abundant in leafy greens, nuts, beans, and whole grains, helps regulate blood pressure and supports healthy vascular tone, both directly relevant to hemorrhagic stroke prevention.
Why Women May Benefit More Than Men
The California Teachers Study was conducted exclusively in women, and the findings raise an important question: does the Mediterranean diet offer women specifically enhanced stroke protection? Several lines of evidence suggest it does, and the reasons involve the intersection of hormonal biology, vascular aging, and inflammatory pathways that differ between the sexes.
After menopause, estrogen levels decline sharply. Estrogen normally acts as a potent neuroprotector, supporting blood vessel elasticity, reducing oxidative stress, and suppressing the inflammatory molecules that drive atherosclerosis. When estrogen declines, women’s blood vessels become more vulnerable to inflammation-driven damage. This vulnerability window coincides with the age range when stroke risk climbs most steeply. The average age of the women in this study was 53 at baseline, meaning the majority transitioned through menopause during the 21-year follow-up period.

The Mediterranean diet’s dense concentration of anti-inflammatory and antioxidant compounds may help fill the protective gap that estrogen loss creates. Polyphenols from olive oil, berries, and vegetables activate some of the same anti-inflammatory pathways that estrogen supports, including suppression of nuclear factor kappa-B (NF-kB), a master regulator of inflammatory gene expression. The diet’s phytoestrogens, found in legumes and flaxseeds, are plant-based compounds structurally similar to estrogen that can weakly bind to estrogen receptors and provide partial hormonal support during the menopausal transition. One intervention study found that women following a Mediterranean diet for six months showed a significant decrease (over 40%) in total estrogen levels, a finding that sounds paradoxical but actually suggests improved estrogen metabolism and reduced exposure to the forms of estrogen associated with increased disease risk.
This hormonal dimension may explain why the hemorrhagic stroke reduction (25%) was so much larger than the ischemic stroke reduction (16%). Hemorrhagic strokes involve blood vessel rupture, and vessel wall integrity depends heavily on the anti-inflammatory and antioxidant status of vascular tissue. Women experiencing the vascular vulnerability of post-menopausal estrogen decline may gain disproportionate benefit from dietary interventions that bolster vascular resilience through alternative biochemical pathways. Separate research has found that women who follow brain-protective diets like the Mediterranean pattern experience more dramatic cognitive benefits than men, suggesting that the female brain may be especially responsive to dietary anti-inflammatory signals during and after the menopausal transition.
The 9-Point Scoring System as a Practical Self-Assessment Tool
One of the most useful aspects of this study for readers is the 9-point Mediterranean diet score itself. Unlike vague dietary advice to “eat healthier” or “follow the Mediterranean diet,” the scoring system provides a concrete, self-testable framework that takes less than five minutes to assess. You can score yourself right now using median-based thresholds adapted for a general population.
Award yourself one point for each statement that is true about your typical weekly eating pattern: you eat whole grain bread or cereals most days; you eat at least two servings of fruit daily; you eat at least three servings of vegetables daily; you eat beans, lentils, or chickpeas at least twice per week; you use olive oil as your primary cooking fat; you eat fish at least twice per week; and you drink alcohol in moderation (one glass of wine with meals, not binge drinking). Then add one point if you eat red meat fewer than three times per week and one point if you consume dairy products in limited amounts (not as a primary protein source). A score of 6 to 9 places you in the same high-adherence category associated with 18% lower stroke risk in this study. A score of 3 to 5 suggests moderate adherence with room for improvement. A score of 0 to 2 suggests you would benefit significantly from shifting toward Mediterranean eating patterns.
This scoring system also compares instructively to other dietary assessment tools used in recent longevity research. The Nordic diet study published in The Journal of Nutrition used a different scoring system, the NNR23 Food-Based Diet Score, which evaluated adherence to Scandinavian dietary guidelines and found a 23% lower all-cause mortality among high-adherence participants. Both studies used population-median-based scoring rather than absolute nutrient thresholds, which makes the results more generalizable across different populations and food environments. The Nordic diet score also penalized high red meat and sugar intake while rewarding whole grains, fish, legumes, and plant foods, revealing a striking overlap in the dietary patterns that protect against chronic disease regardless of cultural origin. The consistent message from both scoring systems is that shifting even a few points higher on these scales correlates with measurably lower disease risk.
What makes the 9-point Mediterranean score particularly practical is its simplicity. You don’t need to count calories, weigh food portions, or track macronutrient ratios. You need to answer nine yes-or-no questions about your broad eating patterns. For readers who have found other dietary assessment tools overwhelming, this binary scoring approach offers a clear entry point for self-evaluation and incremental improvement. Moving from a score of 3 to a score of 5, for example, might require only adding a weekly serving of fish and swapping your cooking oil from vegetable oil to olive oil.
Best Food Sources for Stroke Prevention
The Mediterranean diet’s protective effect comes from the collective action of its food components, not from any single ingredient. But the research points to several categories that carry the heaviest anti-inflammatory and vascular-protective weight. Understanding which foods contribute most allows you to prioritize the changes that deliver the biggest returns.
Olive oil is the dietary cornerstone. Extra-virgin olive oil specifically contains the highest concentration of polyphenols, including hydroxytyrosol and oleocanthal, that reduce vascular inflammation and improve endothelial function. Studies suggest that consuming 2 to 4 tablespoons (30 to 60 ml) of extra-virgin olive oil daily provides meaningful cardiovascular protection. Use it as your primary cooking fat, drizzle it over salads and vegetables, and use it to finish soups and grain dishes.
Fatty fish provides the omega-3 fatty acids EPA and DHA that reduce blood clotting, lower triglycerides, and calm arterial inflammation. The best sources ranked by omega-3 content per serving include Atlantic mackerel, wild salmon, sardines, herring, and anchovies. Target two to three servings (roughly 8 to 12 ounces total) per week, which aligns with both the Mediterranean diet score criteria and the American Heart Association’s recommendations.
Leafy greens and cruciferous vegetables deliver nitrates that the body converts to nitric oxide, a molecule that dilates blood vessels and lowers blood pressure. They also provide folate, which helps regulate homocysteine, an amino acid whose elevated levels are associated with increased stroke risk. Spinach, kale, arugula, broccoli, and Brussels sprouts are top choices. Research on diet quality and heart health consistently identifies vegetable intake as a marker that separates protective dietary patterns from harmful ones, regardless of whether the overall approach is low-carb or low-fat.
Legumes (lentils, chickpeas, black beans, white beans) provide soluble fiber that reduces LDL cholesterol, plant-based protein that reduces reliance on red meat, and magnesium that supports healthy blood pressure. The Mediterranean diet score awards a point for above-median legume consumption, which translates to roughly three to four servings per week.
Nuts and seeds combine healthy fats, fiber, magnesium, and polyphenols in a calorie-dense package. Walnuts are especially notable for their alpha-linolenic acid (ALA) content, a plant-based omega-3. Almonds provide vitamin E, a fat-soluble antioxidant that protects cell membranes from oxidative damage. A small daily handful (about 1 ounce or 28 grams) is sufficient for cardiovascular benefit without excessive calorie intake.

Whole grains (oats, barley, whole wheat, farro, brown rice) provide the soluble and insoluble fiber that feeds beneficial gut bacteria and promotes the production of short-chain fatty acids with systemic anti-inflammatory effects. They also provide steady-release energy that helps maintain stable blood sugar, relevant because insulin resistance and type 2 diabetes are major independent risk factors for stroke. Aim for three to four servings of whole grains daily, which might look like oatmeal at breakfast, whole grain bread at lunch, and farro or brown rice at dinner.
Berries and fruits contribute flavonoids and anthocyanins that protect blood vessels from oxidative damage. Blueberries, strawberries, and grapes are particularly rich in these compounds. Two to three servings of whole fruit per day satisfies the Mediterranean diet score criterion while providing vitamin C, potassium, and additional fiber. As with the cardiovascular benefits of whole-food dietary patterns, the polyphenols in fruits and berries work synergistically with the fats in olive oil and fish to amplify each other’s absorption and biological activity.
A Sample Mediterranean Day for Stroke Prevention
Translating the research into an actual eating pattern is where most nutrition advice falls apart. Here is a sample day that scores 8 or 9 on the Mediterranean diet scale, specifically designed around the food categories most strongly associated with stroke prevention.
Breakfast: Steel-cut oatmeal topped with a handful of blueberries and sliced strawberries, a tablespoon of ground flaxseed, and a drizzle of extra-virgin olive oil. A small glass of water with lemon. This meal covers whole grains, fruit, and healthy fat before 9 AM.
Lunch: A large salad of mixed greens (spinach, arugula, romaine) with chickpeas, cherry tomatoes, cucumber, red onion, Kalamata olives, and a generous olive oil and lemon dressing. A slice of whole grain bread on the side. This adds vegetables, legumes, and additional olive oil.
Afternoon snack: A small handful of walnuts and almonds (about 1 ounce) with an apple or a few dried figs. This provides plant-based omega-3 from walnuts and additional fruit.
Dinner: Grilled salmon (about 5 ounces) with roasted broccoli, a side of lentils seasoned with garlic, lemon, and herbs, and a small glass of red wine if you drink alcohol. Drizzle olive oil over the broccoli and lentils after cooking for maximum polyphenol retention.
Daily totals (approximate): 3 tablespoons extra-virgin olive oil, 5+ servings vegetables, 3 servings fruit, 1 serving fatty fish, 1 serving legumes, 3 servings whole grains, 1 serving nuts. This pattern accumulates 7 or 8 points on the 9-point scale before even accounting for limited red meat and dairy consumption.
What to Eat
The evidence from this 21-year, 105,000-woman study is both clear and actionable. Closely following the Mediterranean dietary pattern reduces stroke risk by 18% overall, with the strongest protection (25% reduction) against hemorrhagic stroke, the deadliest subtype. The biological mechanisms are well established: anti-inflammatory polyphenols from olive oil, omega-3 fatty acids from fish, nitric oxide from leafy greens, and fiber from whole grains and legumes collectively protect blood vessels from the damage that leads to stroke.
Three action steps to implement this week. First, score yourself on the 9-point Mediterranean diet scale described above. Knowing your starting point makes the path forward specific rather than abstract. Most Americans score between 2 and 4, which means even modest improvements (reaching 5 or 6) would move you closer to the protective threshold observed in this study. Second, make two targeted swaps: replace your current cooking oil with extra-virgin olive oil, and replace one or two weekly red meat meals with fatty fish (salmon, mackerel, or sardines). These two changes alone can shift your score by 2 to 3 points and address two of the most potent protective mechanisms identified in the research. Third, add a daily serving of legumes. Toss chickpeas into a salad, blend white beans into a soup, or cook a batch of lentils on Sunday to use throughout the week. Legumes are the most underconsumed food group in the typical American diet, and they tick multiple boxes for stroke prevention: fiber, magnesium, plant protein, and folate.
The study does carry limitations. Dietary information was self-reported through questionnaires completed at baseline, which means eating patterns may have changed during the 21-year follow-up. The cohort consisted of California educators, a population with higher-than-average health literacy and socioeconomic status, which may limit generalizability. And as with all observational research, the results show association rather than direct causation. But the consistency of Mediterranean diet research across dozens of studies, populations, and follow-up periods, combined with well-understood biological mechanisms, makes this one of the most evidence-supported dietary recommendations in all of nutritional science. As Wang concluded, “Improving our diets could lessen our risk for this devastating disease.” For women approaching or past menopause, the case for filling your plate with olive oil, fish, vegetables, legumes, and whole grains has never been stronger.
Sources
- Wang SS, et al. “Mediterranean Diet and the Risk of Stroke Subtypes in Women.” Neurology Open Access, February 4, 2026. https://www.neurology.org/doi/10.1212/WN9.0000000000000062
- American Academy of Neurology. “Mediterranean diet associated with lower risk of all stroke subtypes in women.” Press Release, February 2026. https://www.aan.com/PressRoom/Home/PressRelease/5310
- ScienceDaily. “This popular diet was linked to a much lower stroke risk.” February 9, 2026. https://www.sciencedaily.com/releases/2026/02/260209064310.htm
- Estruch R, et al. “Primary Prevention of Cardiovascular Disease with a Mediterranean Diet Supplemented with Extra-Virgin Olive Oil or Nuts.” New England Journal of Medicine, 2018. https://www.nejm.org/doi/full/10.1056/NEJMoa1800389
- CDC. “Stroke Facts.” Centers for Disease Control and Prevention. https://www.cdc.gov/stroke/data-research/facts-stats/index.html





