
The rise of GLP-1 receptor agonists like semaglutide (Ozempic, Wegovy) and tirzepatide (Mounjaro, Zepbound) has fundamentally transformed the weight management landscape, delivering results that previously required surgical intervention. Clinical trials consistently demonstrate 15-20% body weight reduction over 68 weeks, numbers that seemed almost impossible through lifestyle modification alone. But buried in those impressive statistics lies a concerning pattern that doesn’t make it into the marketing materials: participants in GLP-1 trials lost substantial amounts of lean muscle mass alongside the fat, sometimes accounting for 25-40% of total weight lost.
This isn’t just an aesthetic concern about muscle tone. Lean mass is your metabolic engine, the tissue that burns calories at rest, regulates glucose uptake, maintains functional strength for daily activities, and protects against metabolic dysfunction as you age. A 2024 analysis published in The Lancet Diabetes & Endocrinology found that GLP-1 users who lost significant muscle mass were more likely to regain weight after discontinuing medication and experienced greater declines in resting metabolic rate compared to those who preserved their lean tissue. The medication creates the caloric deficit, but without strategic nutrition, your body may burn the wrong substrate.
The solution isn’t simply “eat more protein.” For GLP-1 users, the challenge is profoundly practical: when appetite is suppressed so dramatically that eating feels like a chore, hitting adequate protein targets becomes genuinely difficult. The answer lies in understanding how these medications alter your physiology and then timing protein intake to work with those changes rather than against them. By restructuring when and how you consume protein, you can protect your metabolic foundation while the medication does its work.
The Physiology of Muscle Preservation
Muscle tissue exists in a constant state of turnover, simultaneously breaking down (muscle protein breakdown, or MPB) and rebuilding (muscle protein synthesis, or MPS). In metabolic equilibrium, these processes balance each other. But when you’re in a significant caloric deficit, as GLP-1 users necessarily are, the breakdown side accelerates while synthesis struggles to keep pace. Your body becomes catabolic, breaking down tissue for energy, and without intervention, muscle becomes collateral damage in the fat-loss process.
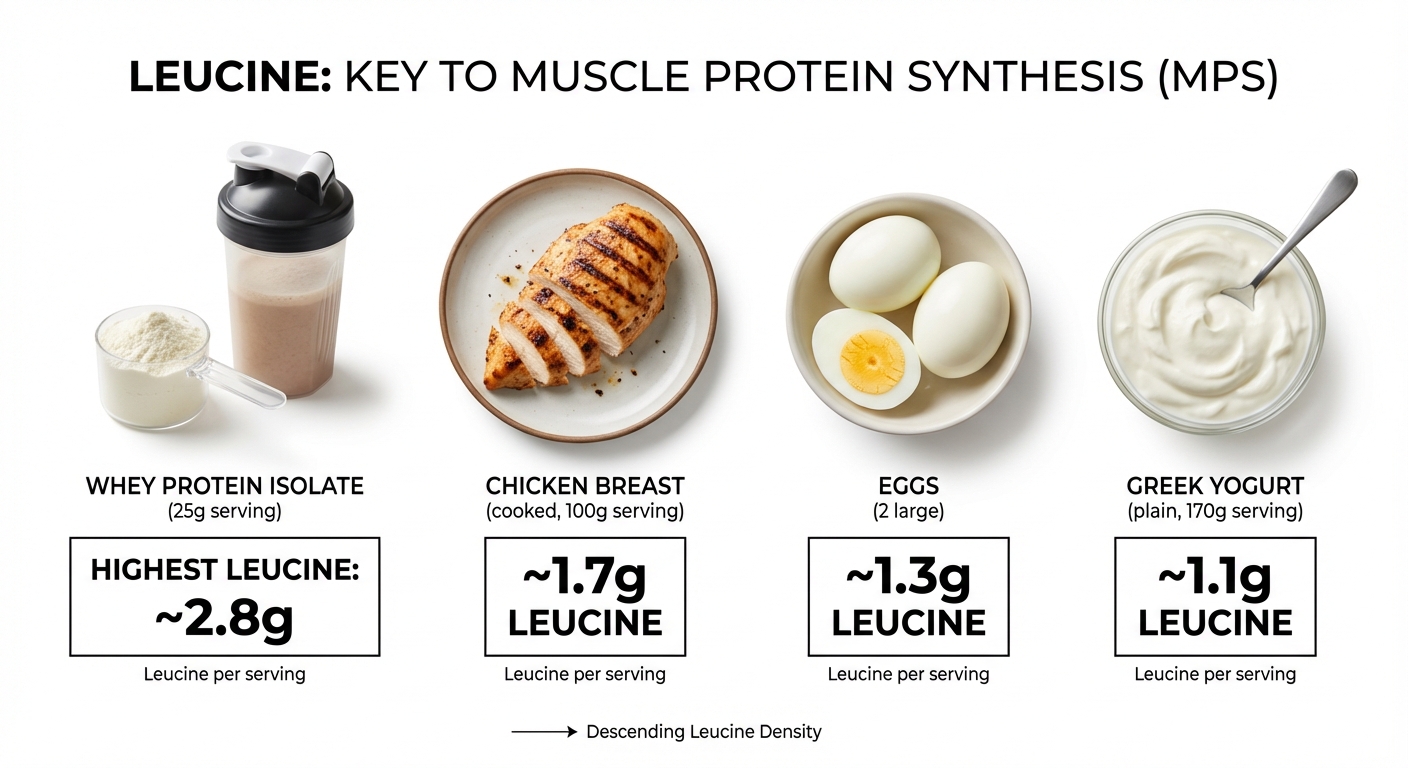
For MPS to occur at meaningful rates, blood levels of the amino acid leucine must cross a specific threshold, typically around 2.5 to 3 grams of leucine per meal, which translates to approximately 25-40 grams of high-quality protein depending on the source. This is the “leucine trigger” that signals muscle cells to begin the anabolic process. Below this threshold, muscle cells don’t receive the biochemical message to rebuild, even if total daily protein intake appears adequate on paper. This is why “grazing” on small amounts of protein throughout the day, common among people who feel too full to eat real meals, may be profoundly counterproductive for muscle preservation.
Dr. Layne Norton, a researcher specializing in muscle metabolism and protein requirements, emphasizes that the distribution of protein throughout the day matters as much as total intake for GLP-1 users. His research suggests that three to four distinct “protein feeding events” per day, each containing enough protein to cross the leucine threshold, produces superior muscle preservation compared to the same total protein consumed in smaller, more frequent doses. For someone targeting 120 grams of protein daily, this means three meals of 40 grams each rather than six snacks of 20 grams, a distribution that may feel counterintuitive but aligns with the underlying biochemistry.
Why GLP-1s Change the Protein Timing Equation
The mechanisms that make GLP-1 medications so effective for weight loss, delayed gastric emptying, enhanced satiety signaling, and reduced food reward sensitivity, simultaneously create unique challenges for protein absorption and utilization. When you eat a meal on semaglutide, that food sits in your stomach considerably longer than normal, sometimes 2-3 times the usual gastric residence time. The amino acids from that meal are released into your bloodstream more gradually, flattening the absorption curve that would normally produce a sharp spike in leucine levels.
This pharmacological alteration effectively mimics a condition called “anabolic resistance” that researchers typically observe in older adults. Normally, a 25-gram dose of protein produces a robust MPS response in young, healthy individuals. But the slowed absorption curve means that leucine may never reach the concentration needed to trigger maximal synthesis, even if the meal contains adequate total protein. A 2023 study in Clinical Nutrition examining protein absorption in patients on GLP-1 therapy found that peak plasma amino acid concentrations were 30-40% lower than expected based on the protein consumed, though the absorption was extended over a longer time period.
The practical implication is straightforward but demanding: GLP-1 users need to consume more protein per meal to achieve the same anabolic stimulus that someone not on the medication would get from a standard serving. Where 25-30 grams per meal might suffice normally, 35-45 grams may be necessary to overcome the flattened absorption curve. This higher per-meal target, combined with the appetite suppression that makes eating difficult, creates the central challenge of nutrition on GLP-1 therapy.
The Bookend Protocol: Strategic Protein Distribution
To navigate these competing demands, nutrition researchers and clinicians working with GLP-1 patients have converged on what might be called the “bookend” approach to protein distribution. Rather than attempting to hit protein targets at every meal, which the medication’s satiety effects make nearly impossible, this strategy prioritizes the first and last meals of the day, creating a framework where even if midday eating falters, the critical windows for muscle preservation are covered.
The morning protein feeding matters because your body wakes in a catabolic state. Overnight fasting depletes liver glycogen and shifts metabolism toward tissue breakdown. Cortisol, the stress hormone that promotes protein degradation, peaks in the early morning hours. A substantial protein intake at breakfast blunts this catabolic signaling, stabilizes blood glucose, and provides the amino acids needed to shift back toward anabolic metabolism. For GLP-1 users, breakfast often represents the best opportunity to hit a high protein target because appetite suppression typically intensifies as the day progresses, especially on higher medication doses.

The evening protein feeding addresses a different physiological window. During deep sleep, the body enters its most active repair phase, releasing growth hormone and directing resources toward tissue maintenance. A slow-digesting protein source before bed provides a sustained amino acid supply throughout this recovery period, minimizing overnight muscle breakdown. Casein protein, the primary protein in dairy, is particularly well-suited for this purpose because its gel-forming properties in the stomach create a time-release effect. A meta-analysis published in Frontiers in Nutrition (2024) found that pre-sleep protein consumption of 30-40 grams significantly improved overnight muscle protein balance in both athletes and clinical populations.
Between these bookend meals, GLP-1 users can relax their protein expectations somewhat. If lunch becomes a few bites of salad because appetite simply isn’t there, the morning and evening feedings provide a safety net. This psychological reframing, from “I must hit protein targets at every meal” to “I must protect my bookends,” reduces the anxiety many patients feel about not eating enough while still maintaining the muscle-preserving structure.
Practical Protein Targets and Food Selection
The question of “how much protein” for GLP-1 users depends on individual factors, but the clinical consensus has shifted toward higher targets than previously recommended. Current guidelines from the American Society for Metabolic and Bariatric Surgery suggest 1.2-1.5 grams of protein per kilogram of ideal body weight for patients on anti-obesity medications, with some researchers advocating for 1.6-2.2 g/kg for those prioritizing muscle preservation. For a person with a goal weight of 70 kg (154 lbs), this translates to approximately 84-154 grams of protein daily, with 100-120 grams being a reasonable middle-ground target.
Achieving these targets when appetite is suppressed requires strategic food selection focused on protein density, the ratio of protein to total volume and calories. High-volume, low-protein foods typically recommended for weight loss, like large salads or air-popped popcorn, may actually be counterproductive for GLP-1 users because they occupy precious stomach space without delivering meaningful protein. The focus should shift to “efficient” proteins that deliver maximum amino acids in minimum volume.
| Protein Source | Protein (g) | Volume/Effort | Leucine (g) | Best Application |
|---|---|---|---|---|
| Whey protein isolate (1 scoop) | 25-27 | Very low | 2.7-3.0 | Breakfast smoothie, post-workout |
| Egg whites (1 cup liquid) | 26 | Low | 2.2 | Breakfast scramble, added to oatmeal |
| Greek yogurt (1 cup, 0% fat) | 20-23 | Medium | 1.8 | Pre-bed snack, breakfast bowl |
| Chicken breast (4 oz) | 35 | High (requires cooking) | 2.5 | Lunch or dinner main |
| Cottage cheese (1 cup) | 25-28 | Low | 2.4 | Snack, breakfast option |
| Casein protein (1 scoop) | 24 | Very low | 2.2 | Pre-bed shake |
For many GLP-1 users, liquid nutrition becomes not optional but essential. Drinking calories often carries negative connotations in the weight-loss world, but for patients struggling to eat solid food due to medication-induced satiety, protein shakes and smoothies may be the only practical way to hit targets. A morning shake with 1.5 scoops of whey isolate, Greek yogurt, and a tablespoon of nut butter can deliver 45-50 grams of protein in a format that many patients tolerate far better than an equivalent solid meal.
The Hydration Imperative
An often-overlooked aspect of high-protein nutrition on GLP-1 medications is the increased demand for hydration. Protein metabolism generates nitrogenous waste products (urea, ammonia) that must be filtered by the kidneys and excreted in urine. Higher protein intakes naturally increase this metabolic burden, requiring additional water to process effectively. Compounding this issue, GLP-1 receptor agonists appear to reduce thirst signaling in the hypothalamus, meaning patients often don’t feel thirsty even when objectively dehydrated.
Dehydration doesn’t just cause the obvious symptoms of fatigue and headache. It directly impairs muscle protein synthesis through mechanisms involving reduced blood flow to muscle tissue and altered cellular signaling. A 2022 study in the European Journal of Applied Physiology found that even mild dehydration (2% body mass loss) reduced the anabolic response to protein ingestion by approximately 20%. Your careful protein strategy can be partially undermined simply by not drinking enough water.
The target for most GLP-1 users should be 2.5 to 3.5 liters of total fluid daily, with increased intake during exercise or hot weather. Adding electrolytes becomes particularly important for those also following a lower-carbohydrate approach, as reduced insulin levels promote sodium excretion by the kidneys. Symptoms like muscle cramps, lightheadedness upon standing, or persistent fatigue despite adequate sleep often indicate an electrolyte imbalance rather than a medication side effect.
Sample Day: Protein-Optimized GLP-1 Nutrition
Breakfast (7:00 AM): Target 40-45g protein Protein smoothie: 1.5 scoops whey isolate (38g), 1/2 cup Greek yogurt (10g), 1 tbsp almond butter (4g), 1 cup unsweetened almond milk, 1/2 cup frozen berries. Total: ~52g protein in a drinkable format.
Midday (12:30 PM): Target 20-30g protein (flexible) If appetite allows: 4 oz grilled chicken (35g) on a small salad. If appetite is minimal: 1 cup cottage cheese (25g) eaten over an hour. If eating feels impossible: skip and protect the evening window.
Evening (6:30 PM): Target 35-40g protein 5 oz salmon (33g) with roasted vegetables. Or if solid food is difficult: scrambled egg whites (26g) with 1 oz cheese (7g).
Pre-bed (9:30 PM): Target 25-30g protein 1 cup Greek yogurt (20g) with 1/2 scoop casein (12g) mixed in. Or a casein shake with almond milk.
Daily Total: 115-135g protein depending on midday intake, with essential windows protected regardless of appetite fluctuations.
The Bottom Line
GLP-1 medications are transformative tools for weight loss, but without deliberate protein strategy, they can inadvertently undermine your metabolic health by promoting excessive muscle loss. The key adaptations for GLP-1 users are higher per-meal protein targets to overcome slowed absorption, strategic “bookend” timing that prioritizes breakfast and pre-sleep feeding, and a willingness to use liquid nutrition when solid food intake is impaired by medication effects.
Next Steps:
- Calculate your protein target: goal weight in kg × 1.6 = minimum daily grams
- Audit your current protein intake for three days to establish baseline
- Restructure to prioritize 35-45g protein at breakfast
- Add pre-bed casein or Greek yogurt (25-30g protein)
- Track hydration alongside protein, targeting 3+ liters daily
For related guidance, explore the benefits of daily walking for metabolic health, which pairs well with protein optimization on GLP-1 therapy. If you’re also incorporating exercise, our strength training after 50 guide covers resistance training approaches that synergize with protein optimization.
Sources: The Lancet Diabetes & Endocrinology (2024, GLP-1 and lean mass), Clinical Nutrition (2023, protein absorption in GLP-1 therapy), Dr. Layne Norton research on protein distribution and leucine threshold, Frontiers in Nutrition (2024, pre-sleep protein meta-analysis), American Society for Metabolic and Bariatric Surgery protein guidelines, European Journal of Applied Physiology (2022, dehydration and MPS).





