
When the conversation turns to winter supplementation, vitamin D monopolizes the attention. This isn’t unwarranted; vitamin D deficiency is endemic in northern latitudes during winter months, and its implications for immune function, bone health, and mood are well-documented. But the singular focus on D3 obscures a more complex reality: winter conditions affect the status of multiple micronutrients, and these nutrients interact with each other in ways that make isolated supplementation less effective than comprehensive optimization.
The seasonal shifts that reduce vitamin D synthesis also alter eating patterns, physical activity, and sun exposure in ways that affect other nutritional parameters. Reduced fresh produce availability and consumption in winter months affects vitamin C and certain B vitamins. Decreased outdoor activity affects not just vitamin D but also the electrolytes lost through sweat. The stress of holiday seasons depletes magnesium. Each deficiency or insufficiency creates downstream effects that isolated supplementation cannot fully address.
This guide takes a systems approach to winter micronutrient optimization, addressing the most common deficiencies and insufficiencies, their interactions, and practical supplementation protocols based on current research. The goal isn’t to sell you on a list of pills but to help you understand what your body actually needs during winter months and how to meet those needs efficiently.
Vitamin D: The Foundation That Everyone Discusses
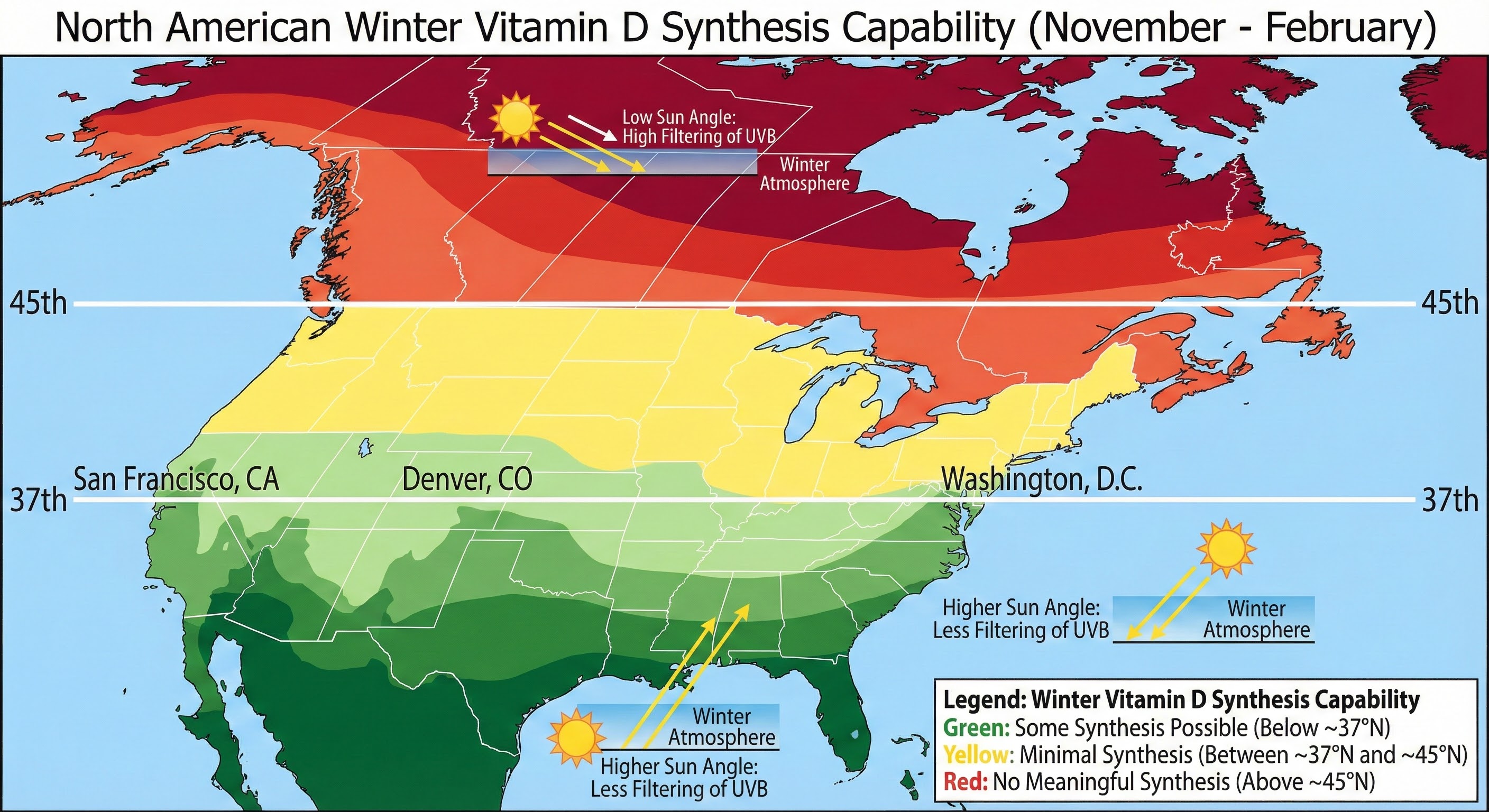
Vitamin D deserves its prominence in winter health discussions because the problem is nearly universal in temperate climates. Above the 37th parallel (roughly the latitude of San Francisco or Washington, DC), the winter sun angle is so low that even prolonged outdoor exposure fails to trigger meaningful vitamin D synthesis in the skin. You could stand shirtless in the noon sun on a December day in Boston and synthesize essentially no vitamin D, as the UVB rays necessary for conversion are filtered out by the atmosphere at that angle.
Blood levels of 25-hydroxyvitamin D, the standard marker for vitamin D status, should ideally fall between 40 and 60 ng/mL for optimal function. The average American in winter hovers around 20 to 30 ng/mL, with many falling into outright deficiency below 20 ng/mL. This isn’t a subtle insufficiency; it’s a significant gap between actual and optimal status that affects immune function, bone metabolism, muscle function, and mood.
Supplementation requirements depend heavily on baseline status, body composition, and individual absorption. Heavier individuals require more vitamin D because it’s fat-soluble and distributes into adipose tissue. People with darker skin require more because melanin reduces synthesis efficiency. Those with absorption issues need higher doses to achieve the same serum levels. Testing before supplementation establishes your baseline and allows for targeted dosing rather than guesswork.
General guidance for those without testing suggests 2,000 to 5,000 IU of D3 daily during winter months, with the higher end appropriate for those with higher body weight, darker skin, or minimal sun exposure. D3 (cholecalciferol) is preferred over D2 (ergocalciferol) because it raises serum levels more effectively and maintains them longer. Take it with dietary fat to enhance absorption; the fat-soluble vitamin requires bile secretion for uptake.
Our comprehensive guide on vitamin D optimization covers dosing, testing, and the vitamin D/K2 interaction in greater detail.
Magnesium: The Most Common Deficiency You’ve Never Tested
If vitamin D is the celebrity of winter supplementation, magnesium is the unrecognized workhorse that virtually everyone needs and few adequately address. An estimated 50 to 60 percent of Americans fail to meet the recommended daily intake for magnesium, and blood testing dramatically underestimates deficiency because less than 1 percent of body magnesium circulates in serum.
Magnesium participates in over 300 enzymatic reactions, including those governing muscle function, nerve transmission, blood sugar control, and blood pressure regulation. It’s also essential for vitamin D metabolism; magnesium-dependent enzymes convert vitamin D to its active form. Taking high-dose vitamin D while magnesium-depleted can actually worsen certain symptoms because the increased vitamin D activity depletes magnesium further.
Winter conditions exacerbate magnesium insufficiency through several mechanisms. Holiday stress depletes magnesium, as the mineral is consumed in stress hormone production. Increased alcohol consumption (common during holiday season) increases magnesium excretion through urine. Reduced consumption of leafy greens and nuts, common in winter diets, reduces dietary intake. The result is that by mid-winter, many people are running on substantially depleted magnesium stores.
The recommended daily intake is 400 to 420 mg for men and 310 to 320 mg for women. Most people consume 250 to 300 mg from diet, creating a gap of 100 to 150 mg that supplementation can fill. The form matters significantly: magnesium oxide is poorly absorbed and primarily acts as a laxative, while magnesium glycinate, citrate, and threonate offer superior bioavailability.
Magnesium glycinate is preferred for general supplementation because glycine has calming effects that complement magnesium’s role in nervous system regulation. Magnesium threonate has specific evidence for crossing the blood-brain barrier and may offer cognitive benefits. Magnesium citrate provides good absorption but can have laxative effects at higher doses. Starting with 200 mg of glycinate or citrate at bedtime addresses the deficiency while promoting sleep quality through muscle relaxation.
Omega-3 Fatty Acids: The Anti-Inflammatory Foundation
Omega-3 fatty acids, particularly EPA (eicosapentaenoic acid) and DHA (docosahexaenoic acid) from marine sources, provide anti-inflammatory effects that become particularly valuable during winter months. The combination of reduced physical activity, increased comfort food consumption, and holiday stress creates a pro-inflammatory environment that omega-3s help counterbalance.
The typical Western diet provides far more omega-6 fatty acids than omega-3s, with ratios often exceeding 15:1 or even 20:1. While both families are essential, this imbalance promotes inflammatory signaling. Increasing omega-3 intake helps restore balance, reducing the low-grade systemic inflammation that contributes to conditions ranging from joint pain to depression.
Depression and seasonal mood changes specifically benefit from omega-3 supplementation. Meta-analyses consistently show that EPA-predominant formulations reduce depressive symptoms, likely through modulation of inflammatory pathways and effects on neurotransmitter systems. Winter’s increased depression risk makes this particularly relevant during dark months.
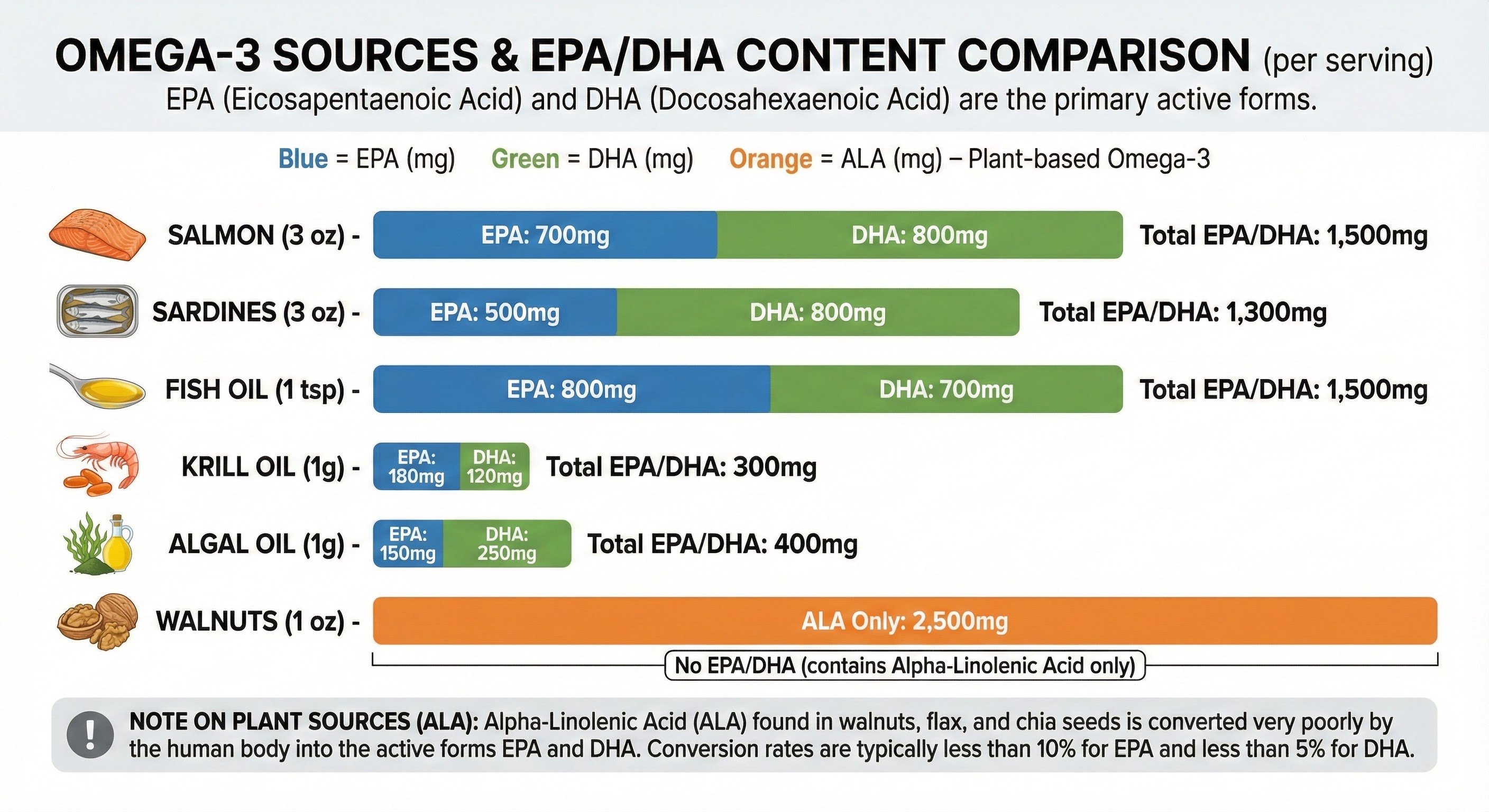
Effective dosing for general health maintenance involves 1,000 to 2,000 mg combined EPA and DHA daily. Those targeting mood support or inflammation may benefit from higher doses of 2,000 to 4,000 mg. Look for products with at least 500 mg EPA and 250 mg DHA per serving, and check for third-party testing that verifies purity and absence of oxidation (rancidity).
Fish oil is the most common source, but algal oil provides a vegan alternative that supplies DHA and increasingly EPA as well. Krill oil offers phospholipid-bound omega-3s with potentially superior absorption, plus astaxanthin, an antioxidant that provides additional benefits. Whichever source you choose, take it with food containing fat to optimize absorption.
Zinc: The Immune Support Mineral
Zinc plays essential roles in immune cell development and function, making adequate status particularly important during winter’s cold and flu season. Zinc deficiency impairs both innate and adaptive immune responses, increasing susceptibility to infections and potentially extending their duration when they occur.
Unlike vitamin D and magnesium, zinc deficiency is less universal but affects specific populations at higher rates. Vegetarians and vegans face increased risk because plant zinc sources have lower bioavailability due to phytic acid binding. Older adults have reduced zinc absorption. Athletes lose zinc through sweat. Heavy alcohol consumers deplete zinc stores.
Acute zinc supplementation at the onset of cold symptoms has modest but consistent evidence for reducing symptom duration. The mechanism involves zinc’s interference with viral replication in the nasopharyngeal mucosa, which is why lozenges that dissolve slowly in the mouth show stronger effects than swallowed capsules. Zinc acetate and zinc gluconate are the best-studied forms for this application.
For prophylactic use during winter, 15 to 30 mg of elemental zinc daily is appropriate for most adults. Higher doses (above 50 mg daily) can interfere with copper absorption and should be avoided for extended periods. Those taking zinc supplements long-term should ensure adequate copper intake, either through diet (shellfish, liver, nuts, seeds) or a modest copper supplement (1-2 mg daily).
Food sources include oysters (by far the richest source), beef, crab, lobster, and pork. Plant sources like pumpkin seeds, chickpeas, and cashews provide zinc but in less bioavailable forms. Combining plant zinc sources with vitamin C-containing foods improves absorption.
Vitamin C: Beyond the Cold Myth
Vitamin C’s reputation as a cold-fighter is exaggerated in popular culture but not entirely without foundation. The research is clear that vitamin C doesn’t prevent colds in the general population, but it may modestly reduce duration (by about 8 percent in adults) and shows stronger effects in people under physical stress, including cold exposure.
More relevant to winter wellness is vitamin C’s role as an antioxidant and cofactor for collagen synthesis, immune cell function, and iron absorption. The stress of holiday season increases vitamin C requirements, as stress hormones consume vitamin C in their synthesis. Reduced fresh produce consumption in winter further challenges intake.
The recommended daily allowance of 75 to 90 mg is easily met through diet if you consume fruits and vegetables, but optimal intake for health benefits may be higher. Research on immune function and antioxidant protection suggests benefits at intakes of 200 to 500 mg daily. Above this level, absorption efficiency drops and excess is excreted in urine, making megadosing inefficient rather than harmful.
Rather than a single large dose, dividing vitamin C intake across the day makes better use of absorption capacity. A modest supplement (250-500 mg) plus vitamin C-rich foods (citrus, bell peppers, strawberries, broccoli) distributed across meals optimizes intake. Those with limited fresh produce access in winter may benefit from higher supplementation.
The B-Complex: Energy and Mood Support
The B vitamins function as a family, with deficiencies in any single member affecting the metabolism of others. Winter’s combination of reduced activity, altered eating patterns, and increased stress can challenge status of several B vitamins simultaneously, making a comprehensive approach more practical than isolated supplementation.
B12 deficiency specifically affects vegetarians, vegans, and older adults with reduced intrinsic factor production. The fatigue and cognitive symptoms of B12 deficiency can mimic or exacerbate seasonal depression, making adequate status particularly important during dark winter months. Those in risk groups should test and supplement as needed.
Folate (B9) works closely with B12 in methylation pathways that affect neurotransmitter synthesis. Low folate status is associated with depression and may contribute to winter mood challenges. The active form, methylfolate, is preferred over folic acid for supplementation because it bypasses the MTHFR polymorphism that affects folic acid processing in a substantial portion of the population.
A quality B-complex supplement containing methylated forms of B12 (methylcobalamin or adenosylcobalamin) and folate (methylfolate) provides comprehensive support. Look for products with adequate doses (at least 400 mcg methylfolate, 100+ mcg B12) rather than token amounts often included in multivitamins.
Vitamin K2: The D3 Partner
Vitamin K2 rarely gets standalone attention but becomes essential when supplementing vitamin D, particularly at higher doses. Vitamin D increases calcium absorption from the gut, but vitamin K2 directs that calcium to appropriate destinations (bones and teeth) rather than inappropriate ones (arterial walls and soft tissues).
Without adequate K2, high-dose vitamin D supplementation theoretically could contribute to vascular calcification. The research here is still developing, but the theoretical mechanism is sound and the precautionary case for K2 co-supplementation is strong. The risk is low and the potential benefit is meaningful, making K2 a reasonable addition to any D3 protocol.
The MK-7 form of K2, derived from natto (fermented soybeans), has the longest half-life and most evidence for bone and vascular benefits. Doses of 100 to 200 mcg daily are commonly recommended alongside D3 supplementation. Some D3 products now include K2 in the formulation, simplifying the protocol.
Those taking blood-thinning medications (warfarin/Coumadin) should consult their physician before adding K2, as it can affect medication dosing. Other anticoagulants like apixaban or rivaroxaban are less affected but still warrant medical consultation.
Testing and Personalization
Generic supplementation protocols address the most common deficiencies but cannot account for individual variation. Testing provides personalized information that transforms supplementation from guesswork to targeted intervention.
Vitamin D testing (25-hydroxyvitamin D) is inexpensive and widely available, establishing baseline status and allowing for dose adjustment. Target levels of 40-60 ng/mL are reasonable for most people. Testing 2-3 months after initiating supplementation confirms whether your dose is achieving the target.
Omega-3 testing through an omega-3 index test measures EPA and DHA as a percentage of red blood cell membrane fatty acids. An index above 8 percent is associated with reduced cardiovascular and cognitive risk. Testing before and after supplementation confirms that your chosen source and dose are producing results.
Magnesium testing is less useful because serum levels poorly reflect tissue status. RBC magnesium is slightly better but still imperfect. Given the high prevalence of insufficiency and the low risk of supplementation, most people can reasonably supplement without testing.
B12 and folate testing is valuable for those in risk groups (vegetarians, vegans, older adults, those with absorption issues). Methylmalonic acid (MMA) provides a more sensitive marker of B12 status than serum B12 alone.
Building Your Winter Protocol
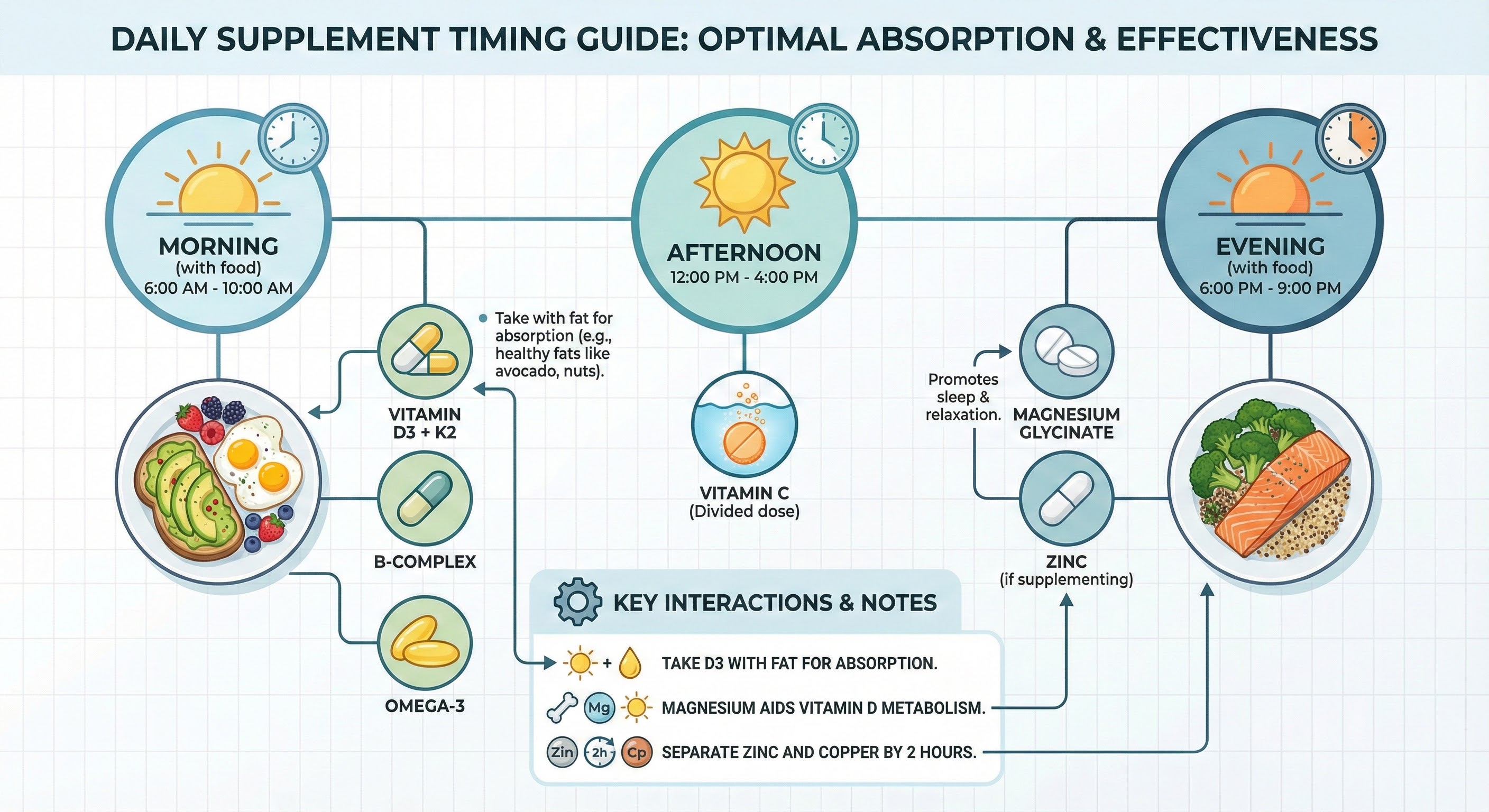
A practical winter supplementation protocol balances comprehensiveness with simplicity. Too many pills leads to poor adherence; too few may leave gaps. The following protocol addresses the most common winter deficiencies with evidence-based doses:
Morning, with breakfast containing fat:
- Vitamin D3: 2,000-5,000 IU (based on baseline status and risk factors)
- Vitamin K2 (MK-7): 100-200 mcg
- Omega-3 (EPA/DHA): 1,000-2,000 mg
- B-complex with methylated forms
Evening, with dinner:
- Magnesium glycinate: 200-400 mg
- Zinc: 15-30 mg (if not meeting needs through diet)
As needed throughout day:
- Vitamin C: 250-500 mg (can divide across meals)
This protocol addresses the most evidence-supported winter deficiencies while remaining manageable. Individual adjustments based on testing, dietary intake, and specific health goals can refine it further.
The Bottom Line
Vitamin D deserves its prominence in winter supplementation discussions, but it’s one component of a multi-nutrient system that winter conditions challenge. Magnesium, omega-3 fatty acids, zinc, vitamin C, and B vitamins all face increased demands or decreased intake during winter months. A comprehensive approach addressing multiple nutrients produces better results than fixating on any single supplement.
Testing transforms generic recommendations into personalized protocols. At minimum, vitamin D testing establishes baseline status and confirms that supplementation is achieving target levels. Those with specific risk factors or health goals may benefit from additional testing. For comprehensive winter wellness, combine supplementation with sleep optimization and anti-inflammatory eating patterns.
Quality matters in supplementation. Bioavailable forms (D3 over D2, methylated B vitamins, chelated minerals) produce better results than their cheaper alternatives. Third-party testing verifies that products contain what they claim and are free from contaminants.
Your Winter Supplement Protocol:
- Test vitamin D and establish baseline; supplement 2,000-5,000 IU D3 daily with K2
- Add magnesium glycinate (200-400 mg) at bedtime for most adults
- Include omega-3s (1,000-2,000 mg EPA/DHA) for anti-inflammatory and mood support
- Consider zinc (15-30 mg) during cold season, especially if dietary intake is low
- Maintain vitamin C through diet plus modest supplementation (250-500 mg)
- Use a quality B-complex with methylated forms if dietary intake is uncertain
Sources: Journal of Clinical Endocrinology & Metabolism vitamin D research, National Institutes of Health Office of Dietary Supplements, American Journal of Clinical Nutrition magnesium status studies, Prostaglandins Leukotrienes and Essential Fatty Acids omega-3 meta-analyses, Cochrane Review zinc and common cold analysis.





