You’re 79 years old, living in Wales, and September 1, 2013, changes everything about your cognitive future. Not because of anything you did, but because of a birthday. If you turned 79 before that date, you qualified for a free shingles vaccine. If you turned 80, you didn’t. This arbitrary cutoff date created one of the most compelling natural experiments in dementia research history, and what researchers found is reshaping how we think about protecting the aging brain.
A team led by Dr. Pascal Geldsetzer at Stanford Medicine analyzed health records from over 280,000 Welsh adults and discovered that those who received the shingles vaccine were 20% less likely to develop dementia over the following seven years. The findings, published in Nature in April 2025 and expanded upon in Cell this month, suggest that a routine vaccination already available at your local pharmacy may offer meaningful protection against one of medicine’s most devastating conditions.
The implications extend beyond prevention. In a follow-up analysis, researchers found that among people already diagnosed with dementia when the vaccine program began, those who received the shot were nearly 30% less likely to die from the disease. “This really suggests the shingles vaccine doesn’t have only preventive, delaying benefits for dementia, but also therapeutic potential,” Geldsetzer noted.
Why Wales Created the Perfect Natural Experiment
Understanding why this study carries such weight requires appreciating what makes the Welsh data so extraordinary. Most vaccine studies suffer from what researchers call “healthy vaccine bias.” People who proactively seek out vaccinations tend to be healthier, better educated, and more engaged with the healthcare system, making it difficult to separate the vaccine’s effects from the characteristics of people who choose to get vaccinated.
The Welsh policy eliminated this problem entirely. The government’s vaccine rollout used birth dates to determine eligibility, not patient choice or health status. Two people born one week apart, living in the same neighborhood, with identical health profiles, faced different eligibility based solely on which side of September 1, 1934, their birthday fell. “What makes the study so powerful is that it’s essentially like a randomized trial with a control group,” Geldsetzer explained.
When researchers examined the two groups, they found them indistinguishable in every measurable characteristic. Education levels, other vaccination rates, chronic disease diagnoses, socioeconomic status, all matched. The only difference was whether they received the shingles vaccine. And the only difference in outcomes was a dramatic drop in dementia diagnoses among the vaccinated group.

The finding wasn’t a fluke. Geldsetzer’s team replicated their analysis using health records from England, Australia, New Zealand, and Canada. In every dataset, the same pattern emerged. “This huge protective signal was there, any which way you looked at the data,” he said.
The Virus in Your Nerves: Understanding the Connection
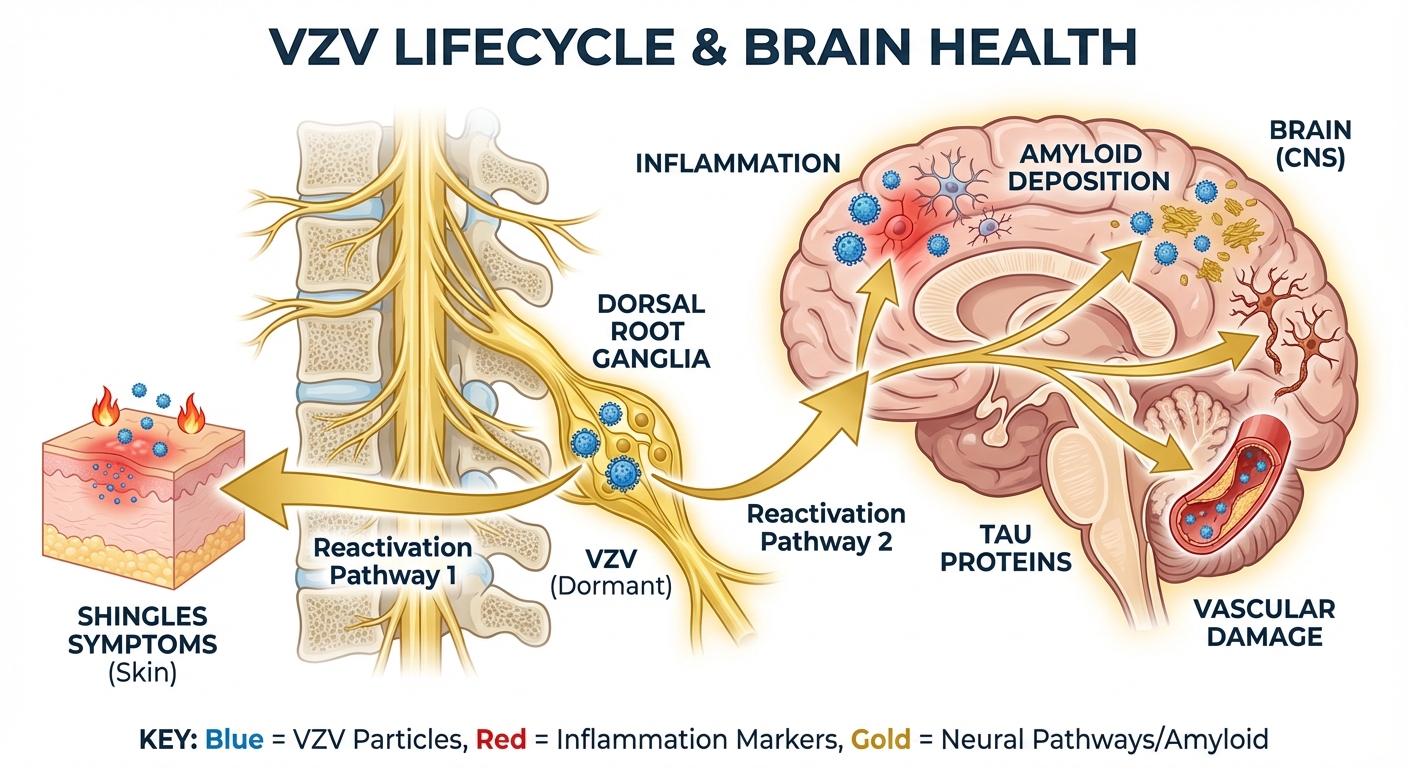
The varicella-zoster virus, or VZV, causes two distinct diseases. In childhood, it manifests as chickenpox. The immune system eventually clears the active infection, but the virus doesn’t leave. Instead, VZV retreats into nerve cells near the spine and brain, where it can remain dormant for decades. In about one-third of people who had chickenpox, the virus eventually reactivates, traveling along nerve fibers to the skin and causing the painful, blistering rash known as shingles.
What researchers have increasingly recognized is that VZV reactivation doesn’t just cause skin symptoms. Even subclinical reactivations, those that never produce visible shingles, may damage neural tissue and trigger inflammatory cascades in the brain. Large-scale analysis of health records from over 100 million Americans published in Nature Medicine found consistent associations between VZV reactivation and subsequent dementia, even after controlling for nearly 400 measured health characteristics.
The mechanisms are multiple and interconnected. VZV reactivation causes vasculopathy, inflammation of blood vessels that supply the brain. It promotes amyloid deposition, the protein plaques characteristic of Alzheimer’s disease. It triggers aggregation of tau proteins, another hallmark of neurodegeneration. And it may activate the herpes simplex virus-1 (HSV-1), which often co-resides in neural tissue and has its own associations with dementia risk.
One particularly intriguing finding suggests that shingles vaccination may provide neuroprotection through pathways beyond just preventing VZV reactivation. Studies of vaccines containing the AS01 adjuvant, an immune-stimulating compound, found similar dementia risk reductions regardless of which pathogen the vaccine targeted. This raises the possibility that robust immune stimulation in older adults may itself confer cognitive benefits, perhaps by enhancing the brain’s ability to clear cellular debris or by modulating inflammatory processes that contribute to neurodegeneration.
Shingrix vs. Zostavax: Does the Newer Vaccine Work Better?
The Welsh natural experiment studied Zostavax, a live-attenuated vaccine introduced in 2006 that has since been phased out in most countries. The current standard, Shingrix, uses a different approach, delivering only specific viral proteins along with the AS01 adjuvant to stimulate immunity. Shingrix prevents shingles in up to 97% of adults aged 50-69, compared to about 51% for Zostavax.
Research published in Nature Medicine suggests that Shingrix may offer even greater dementia protection than its predecessor. Investigators exploited another natural experiment, the transition from Zostavax to Shingrix in the United States in October 2017, to compare outcomes between otherwise similar people who received different vaccines. Those who got Shingrix showed a 17% lower risk of dementia compared to those who received Zostavax, and 23-27% lower risk compared to people who received other vaccines. This translates to 5-9 additional months of dementia-free life.
The enhanced protection might come from Shingrix’s superior ability to prevent VZV reactivation, reducing the cumulative neuroinflammatory burden over time. Alternatively, or additionally, the AS01 adjuvant in Shingrix may provide direct neuroprotective effects. Studies have found that both the AS01-adjuvanted shingles vaccine and the AS01-adjuvanted RSV vaccine showed similar dementia risk reductions, supporting the hypothesis that the adjuvant itself plays a protective role independent of which pathogen it targets.
Who Benefits Most: Surprising Gender Differences
One of the study’s most unexpected findings was a stark difference in vaccine effects between men and women. The protective effect against all-cause dementia and Alzheimer’s disease was substantially stronger in women than in men. For vascular dementia, a form linked to blood vessel damage in the brain, no significant gender difference appeared.
The biological basis for this disparity remains unclear. Women face higher lifetime risk of Alzheimer’s disease than men, a gap only partially explained by women’s longer average lifespans. Hormonal differences, immune system variations, and genetic factors may all contribute. Some researchers speculate that estrogen’s known anti-inflammatory effects may synergize with vaccine-induced immune responses, though this remains speculative.

What’s clear is that the vaccine’s benefits weren’t limited to any single demographic. Across age groups, geographic regions, and baseline health statuses, the protective signal persisted. The consistency of findings across multiple countries and healthcare systems makes confounding unlikely.
Therapeutic Potential: Benefits for Those Already Diagnosed
Perhaps the most surprising finding came from analyzing people who already had dementia when Wales launched its vaccination program. Among this group, those who received the shingles vaccine were nearly 30% less likely to die from dementia during the nine-year follow-up period compared to those who remained unvaccinated.
“We see an effect on your probability of dying from dementia among those who already have dementia,” Geldsetzer explained. “That means that the vaccine doesn’t just have a preventive potential, but actually a therapeutic potential as a treatment.”
The vaccinated group also showed slower progression from mild cognitive impairment to full dementia. This suggests that even after neurodegeneration has begun, reducing VZV reactivation or modulating immune responses may slow the disease course. The mechanism might involve reducing ongoing neuroinflammation, preventing additional viral damage to already compromised brain tissue, or enhancing immune clearance of pathological proteins.
These findings have prompted calls for randomized controlled trials specifically testing whether shingles vaccination can serve as a dementia treatment. Geldsetzer is actively seeking philanthropic funding for such a trial, noting that the live-attenuated vaccine is off-patent and inexpensive, but pharmaceutical companies have little financial incentive to fund studies on generic products.
What This Means for You: Practical Recommendations
The evidence supporting shingles vaccination for brain health joins already compelling reasons to get the shot. Shingles itself causes severe pain lasting weeks to months, and in about 10-18% of cases, leads to postherpetic neuralgia, chronic nerve pain that can persist for years. The vaccine also appears to reduce cardiovascular risk, with vaccinated individuals showing 27% lower risk of blood clots and 25% lower risk of heart attack or stroke.
The CDC recommends Shingrix for all adults 50 years and older, regardless of whether they remember having chickenpox or previously received the older Zostavax vaccine. The vaccine requires two doses, administered 2-6 months apart. Common side effects include injection site pain, fatigue, and muscle aches, typically resolving within 2-3 days.

For those with cognitive concerns in their family history or who simply want to optimize their brain health as they age, the shingles vaccine now represents one of the few interventions with strong evidence for dementia risk reduction. Unlike many proposed dementia preventatives that have failed in clinical trials, this one already exists, is widely available, and addresses multiple health risks simultaneously.
The Bottom Line
A vaccination policy quirk in Wales accidentally revealed what may be one of the most accessible dementia prevention tools we have. The shingles vaccine, already recommended for adults 50 and older, appears to reduce dementia risk by approximately 20%, with the newer Shingrix vaccine potentially offering even greater protection. For those already experiencing cognitive decline, vaccination may slow disease progression and extend survival.
The biological mechanisms likely involve preventing varicella-zoster virus reactivation and its downstream effects on brain inflammation, blood vessel damage, and protein aggregation. Additional protection may come from the vaccine’s adjuvant stimulating beneficial immune responses independent of the targeted pathogen.
Next Steps:
- If you’re 50 or older and haven’t received Shingrix, schedule your first dose with your healthcare provider or pharmacist
- If you received the older Zostavax vaccine, the CDC recommends getting Shingrix anyway for enhanced protection
- Complete the two-dose series, with the second shot 2-6 months after the first
- For those with family history of dementia, discuss comprehensive brain health strategies with your physician, understanding that vaccination is one piece of a larger prevention puzzle
For more on protecting your brain health as you age, see our guides on the critical window between ages 45-55, cognitive nutrition strategies, and evidence-based longevity practices.
Sources: Stanford Medicine, Nature (April 2025), Cell (December 2025), Nature Medicine (2025), CIDRAP, Harvard T.H. Chan School of Public Health, University of Oxford research, ScienceDaily.