You recovered from COVID months ago. The fever broke, the cough disappeared, and your rapid test finally showed a single line. Yet something isn’t right. The fatigue that settled in during your acute illness never left. You struggle to find words that once came easily. Some mornings, the brain fog is so thick that even simple tasks feel overwhelming. Your doctor runs tests, finds nothing conclusive, and you’re left wondering if you’re imagining it all.
You’re not. And the explanation may lie not in SARS-CoV-2 itself, but in a virus you’ve carried since childhood that COVID woke from its decades-long slumber.
A landmark review published in eLife this December by a 17-member NIH Microbiology Task Force has identified viral reactivation as a critical mechanism driving long COVID symptoms. The research reveals that Epstein-Barr virus (EBV), which lies dormant in approximately 95% of adults, may reactivate when COVID disrupts the immune system. In one study, two-thirds of people with long COVID showed markers of recent EBV activity, and those with more symptoms had significantly higher antibody levels. The implications are profound: that persistent fatigue, brain fog, and cognitive difficulties afflicting an estimated 400 million people worldwide may stem not from COVID’s direct damage, but from opportunistic infections emerging in its wake.
The 95% Problem: A Virus Hiding in Plain Sight
To understand why this discovery matters, you need to appreciate how common and how quiet Epstein-Barr virus typically is. Nearly everyone reading this article carries EBV. Most contracted it during childhood without knowing, experiencing mild symptoms that resolved within weeks. In others, initial infection manifests as infectious mononucleosis, the “kissing disease” that causes extreme fatigue, sore throat, and swollen lymph nodes in adolescents and young adults.
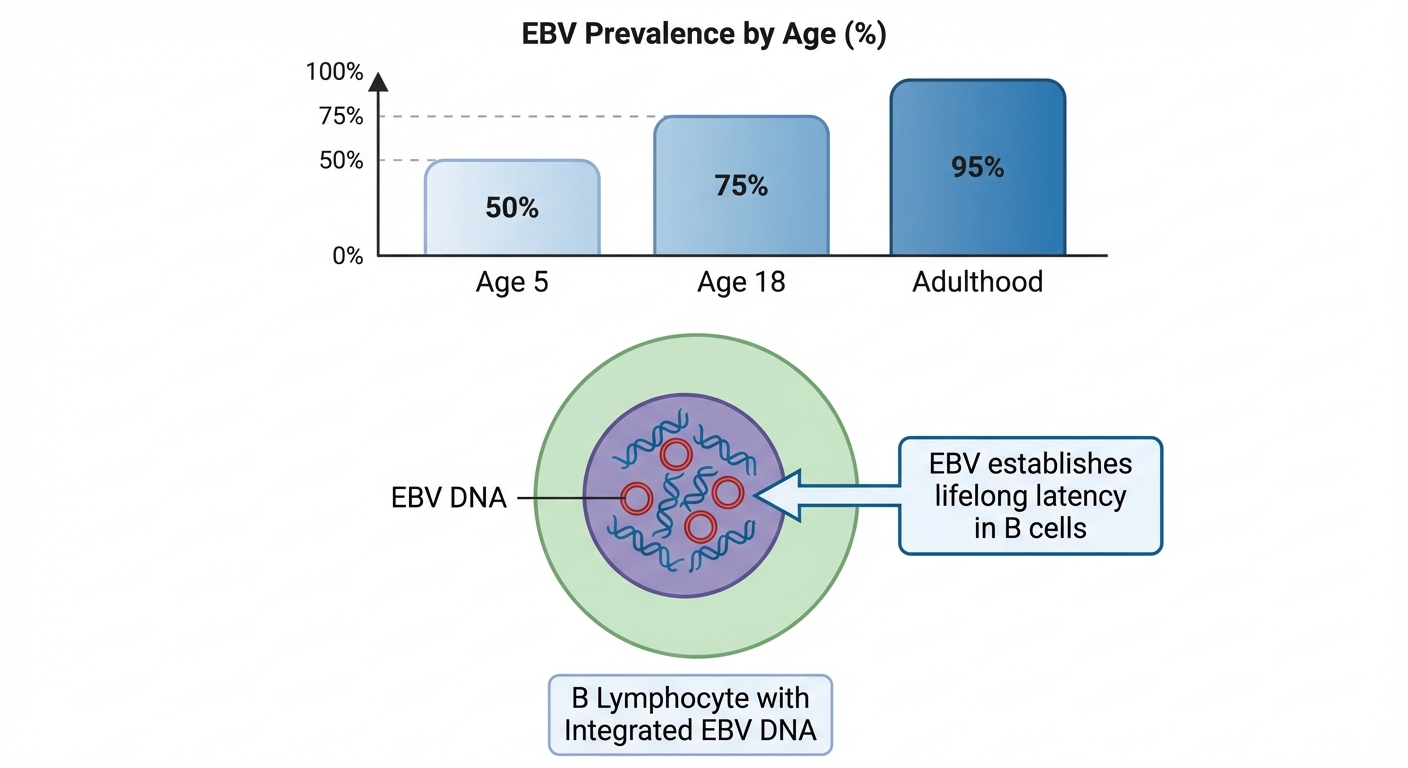
Unlike viruses that your immune system eliminates completely, EBV has evolved a remarkable survival strategy. After acute infection resolves, the virus retreats into B lymphocytes, a type of immune cell, where it integrates its genetic material and enters a dormant state called latency. In this quiet phase, EBV produces minimal proteins, essentially hiding from immune surveillance. A healthy immune system maintains this truce indefinitely, keeping the virus suppressed through constant low-level monitoring.
The problem emerges when that immune surveillance falters. Stress, immunosuppressive medications, other infections, and now, it appears, COVID-19 can disrupt the delicate balance keeping EBV dormant. When the virus reactivates, it begins reproducing and spreading to other cells, triggering an inflammatory response that produces a constellation of symptoms remarkably similar to long COVID: fatigue, cognitive difficulties, sleep disturbance, muscle and joint pain, sore throat, and headaches.
The Two-Thirds Finding: EBV’s Fingerprints on Long COVID
The association between EBV reactivation and long COVID first emerged from a foundational study examining 185 COVID patients. Researchers found that 30.3% developed long COVID symptoms persisting beyond 12 weeks. When they tested for markers of EBV reactivation, the results were striking: 66.7% of long COVID patients showed positive antibody titers indicating recent EBV activity, compared to just 10% of those who recovered normally. The difference wasn’t subtle. It was a six-fold increase.
Subsequent research has expanded and refined these findings. A longitudinal multi-omic study identified four primary risk factors for developing long COVID: type-2 diabetes, SARS-CoV-2 RNA in the blood, specific autoantibodies, and Epstein-Barr virus viremia. EBV wasn’t just associated with long COVID; it was among the strongest predictors of who would develop persistent symptoms.
The symptom specificity is particularly compelling, with cognitive symptoms mirroring issues seen in other conditions affecting brain health and neurotransmitter function. Research has revealed a strong association between EBV reactivation and three specific long COVID manifestations: fatigue, memory deficits, and persistent mucus cough. The odds of developing these symptoms increased by 150% to 250% in those with reactivated EBV. Not all long COVID symptoms showed this association, suggesting that different underlying mechanisms may drive different symptom clusters, with EBV being a primary driver of the debilitating fatigue and cognitive dysfunction that most severely impact quality of life.
How COVID Breaks the Truce: Mechanisms of Reactivation
The exact mechanisms by which SARS-CoV-2 triggers EBV reactivation are still being unraveled, but several pathways have emerged from laboratory and clinical research. Maria Laura Gennaro from Rutgers New Jersey Medical School, who chaired the NIH Microbiology Task Force that produced the December review, emphasized that the timing of co-infections matters significantly. Infections occurring before COVID may weaken existing immunity. Infections during acute illness may intensify tissue damage. Post-recovery infections exploit lingering immune dysfunction.
One concept gaining traction among researchers is “immunity theft,” where acute COVID infection leaves people vulnerable to other infections by depleting or dysregulating immune resources. SARS-CoV-2 has a broad spectrum of cell tropism, effectively infecting epithelial cells throughout the body. While the virus doesn’t directly infect B cells where EBV resides, it creates an environment of immune chaos that allows dormant infections to escape containment.
Laboratory research using EBV-latently-infected epithelial cell lines has demonstrated that SARS-CoV-2 infection can directly trigger EBV reactivation in cells where both viruses co-exist. Epithelial cells lining the respiratory tract, throat, and other tissues can harbor latent EBV, and when COVID infects these same cells, it appears to flip the switch that awakens the dormant virus.
The inflammatory storm that characterizes severe COVID may also play a role. Cytokines, the immune signaling molecules that surge during COVID infection, can themselves trigger viral reactivation. The immune system’s attempt to fight one virus inadvertently provides the signal for another to emerge.
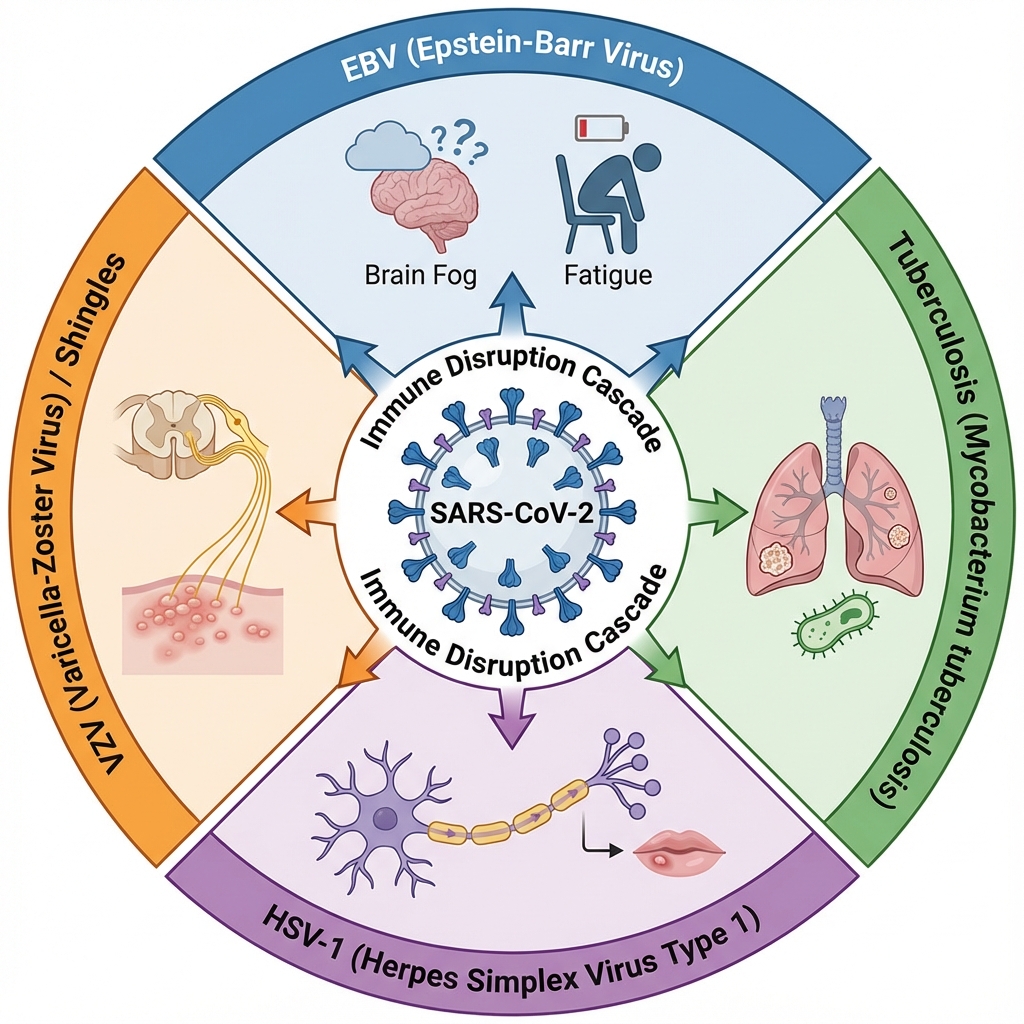
Beyond EBV: The Broader Co-Infection Picture
EBV isn’t the only dormant infection that may reactivate during COVID. The NIH review identified tuberculosis as another potential contributor, noting that approximately one-quarter of the global population carries latent TB. COVID may suppress the specific immune cells that normally contain TB, potentially triggering reactivation in some patients.
The scope of co-infection emergence is global. According to the review, 44 countries experienced tenfold increases in at least 13 infectious diseases during and after the pandemic. Whether these increases reflect COVID-specific immune disruption, pandemic-related healthcare disruptions, or other factors remains an active area of investigation.
Herpes simplex virus-1 (HSV-1), which affects approximately 67% of the global population under age 50, may also reactivate alongside or because of EBV awakening. The two viruses often co-reside in neural tissue, and reactivation of one may trigger the other through shared inflammatory pathways.
The implications extend to understanding long COVID’s heterogeneity. Different patients may have different dormant infections reactivate, or different combinations, potentially explaining why long COVID manifests so variably across individuals. Your particular burden of latent infections, accumulated over a lifetime of exposures, may determine which symptoms you develop when COVID disrupts your immune equilibrium.
The Diagnostic Challenge: Finding the Hidden Infection
One reason viral reactivation has been underappreciated as a long COVID mechanism is that standard testing often misses it. Routine COVID follow-up doesn’t typically include EBV panels, and even when tested, results can be difficult to interpret. EBV antibody patterns are complex, with different antibodies indicating different phases of infection and reactivation.
The most useful markers for identifying recent reactivation are EBV early antigen-diffuse (EA-D) IgG and EBV viral capsid antigen (VCA) IgM. In the foundational study, patients showing these markers were significantly more likely to have long COVID symptoms. Some researchers have also detected EBV DNA in throat washings, with 50% of long COVID patients showing viral shedding compared to 20% of those who recovered normally.
Testing for EBV reactivation in patients with persistent post-COVID symptoms isn’t yet standard practice, but some researchers argue it should be. Early identification might allow for earlier intervention, potentially reducing the intensity and duration of symptoms. At minimum, it could provide validation for patients who struggle to explain why they’re still suffering months after their acute infection resolved.
Treatment Horizons: What Can Be Done
The treatment landscape for EBV reactivation remains frustratingly limited. Unlike some herpesviruses that respond well to antiviral medications, EBV has proven resistant to currently available drugs. As Lawrence S. Young, PhD, a virologist at the University of Warwick, has noted, the antivirals used to treat EBV “are not very effective and better ones are needed.”
Ganciclovir and similar antiherpesvirus agents may offer some benefit, particularly if administered early during reactivation. However, their effectiveness is inconsistent, and they come with significant side effects that limit long-term use. Research into EBV-specific antivirals continues, driven in part by the virus’s association with several cancers and autoimmune diseases, but no breakthrough treatment has yet emerged.
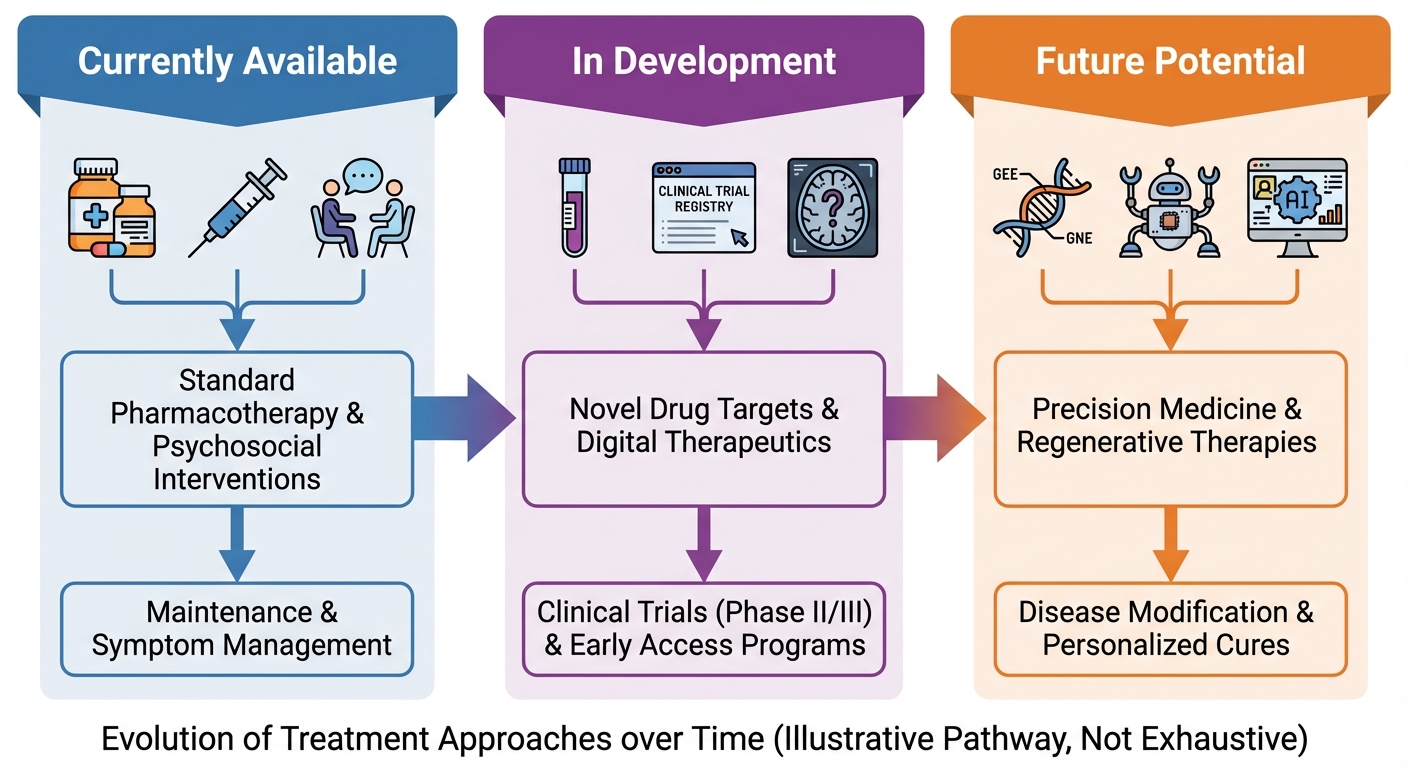
In the absence of targeted antivirals, treatment focuses on supporting immune function and reducing factors that promote viral reactivation. This means addressing the fundamentals: sleep optimization, stress reduction, anti-inflammatory nutrition, and avoiding immunosuppressive exposures when possible. An evidence-based immune support protocol can provide a framework for these foundational interventions. Some practitioners recommend supplements with potential antiviral properties, including zinc, vitamin C, vitamin D for immune optimization, and certain herbal compounds, though evidence for their effectiveness against EBV specifically remains limited.
For patients whose EBV reactivation is confirmed, monitoring symptoms and antibody levels over time can help gauge whether the virus is returning to latency. Many patients do eventually improve as their immune system reestablishes control, though the timeline varies significantly.
The Research Imperative: Causation vs. Correlation
The researchers involved in these studies consistently emphasize an important caveat: correlation doesn’t equal causation. Finding elevated EBV markers in long COVID patients doesn’t prove that EBV reactivation causes their symptoms. It’s possible that whatever immune dysfunction drives long COVID symptoms also, separately, allows EBV to reactivate, with both being consequences of a common underlying mechanism rather than one causing the other.
Establishing causation would require interventional studies showing that suppressing EBV reactivation prevents or treats long COVID symptoms. Such studies are being planned, but they face significant challenges, including the lack of highly effective EBV antivirals and the difficulty of identifying patients early enough in the reactivation process to intervene.
What the evidence does support is that EBV reactivation is a common feature of long COVID, that it’s associated with specific symptom patterns, and that it may represent a treatable component of an otherwise poorly understood syndrome. For the estimated 400 million people worldwide affected by long COVID, even a partial explanation offers hope.
The Bottom Line
The emerging picture of long COVID increasingly includes a role for dormant viral reactivation, with Epstein-Barr virus as the leading suspect. Studies consistently find that two-thirds of long COVID patients show markers of recent EBV activity, with reactivation increasing the odds of fatigue and cognitive symptoms by 150% to 250%. While COVID may be the initial trigger, the persistent symptoms that define long COVID may owe much to viruses we’ve carried since childhood awakening at the worst possible time.
If you’re experiencing persistent fatigue, brain fog, or cognitive difficulties months after COVID infection, consider discussing EBV testing with your healthcare provider. While treatment options remain limited, identifying reactivation can guide supportive care strategies and provide context for your symptoms.
Next Steps:
- Track your symptoms systematically, noting patterns in fatigue and cognitive function
- Discuss EBV antibody testing (EA-D IgG, VCA IgM) with your doctor if symptoms persist beyond 12 weeks
- Prioritize sleep quality and stress management, both of which influence EBV activity
- Consider an anti-inflammatory diet rich in colorful vegetables, fatty fish, and polyphenols
- Stay informed as research progresses; clinical trials targeting viral reactivation are ongoing
Sources: eLife (December 2025), NIH Microbiology Task Force review led by Maria Laura Gennaro (Rutgers), Pathogens journal (Gold et al. 2021), Emerging Microbes & Infections 2025, Dr. Lawrence S. Young (University of Warwick), Nature Medicine co-infection analysis.