A high-fat meal triggers a cascade that most people never feel but that researchers have been studying for decades. Fat molecules enter your bloodstream and interact with immune cells, initiating an inflammatory response that, repeated over years, gradually impairs your cells’ ability to respond to insulin. This chronic low-grade inflammation is now recognized as the primary mechanism driving Type 2 diabetes in most people, not the simple “too much sugar” explanation that dominated thinking for generations. Understanding how to interrupt this inflammatory cascade has become the holy grail of diabetes prevention research, and a study published in Nature Metabolism in December 2025 may have found the key.
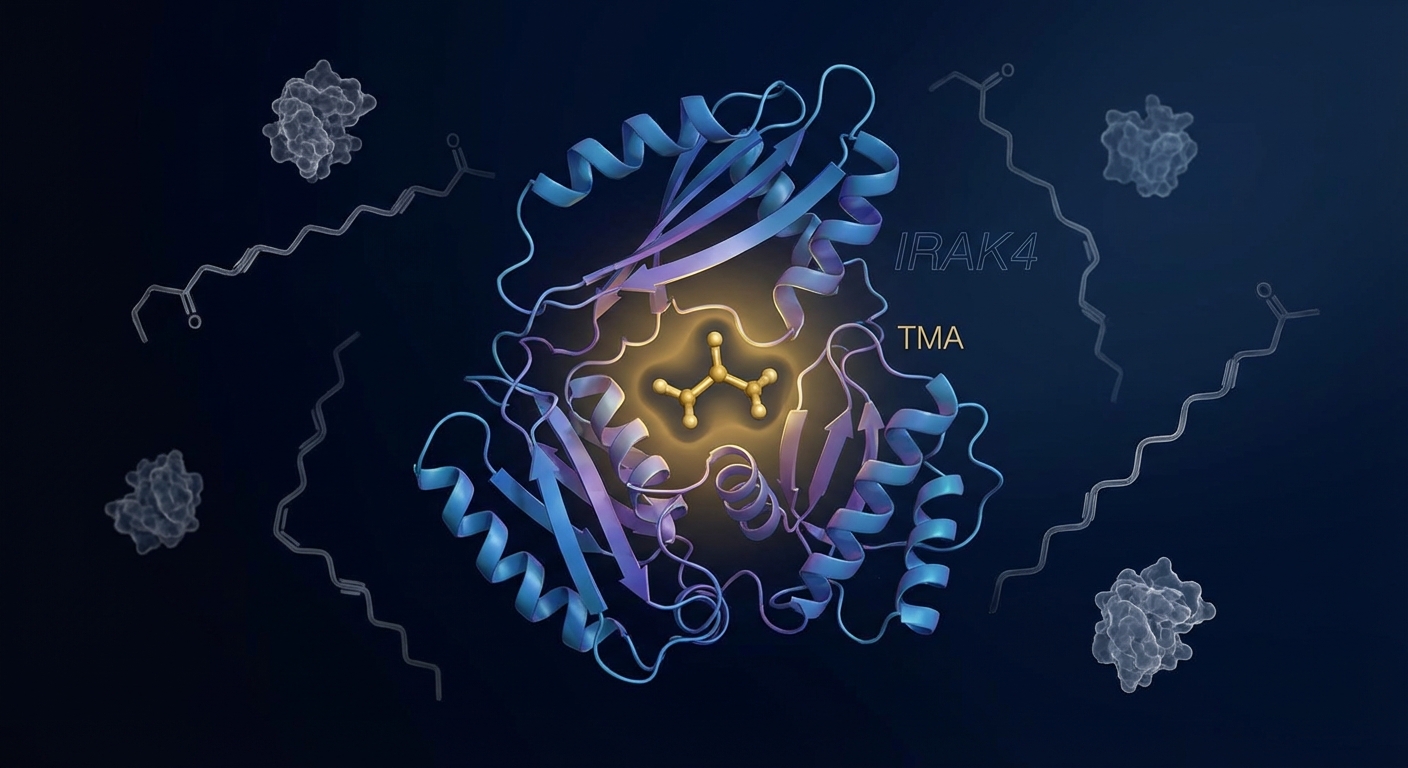
An international team from Imperial College London, the University of Louvain, and the University of Ottawa Heart Institute discovered something unexpected in their investigation of gut-derived metabolites. A compound called trimethylamine, or TMA, produced by certain gut bacteria during the digestion of foods like eggs, fish, and red meat, directly binds to and blocks a critical inflammatory protein called IRAK4. This protein sits at the center of the immune cascade triggered by high-fat diets. By blocking IRAK4, TMA essentially reprograms the inflammatory response to dietary fat, preventing the chronic inflammation that leads to insulin resistance. The implications extend far beyond academic interest: this discovery opens entirely new pathways for preventing and treating Type 2 diabetes.
How Diet-Induced Inflammation Creates Insulin Resistance
To understand why the TMA discovery matters, you need to understand the mechanism it interrupts. When you consume a high-fat meal, particularly one rich in saturated fats, some of those fat molecules interact with toll-like receptors on immune cells throughout your body. These receptors evolved to recognize bacterial invaders, but they also respond to certain fatty acids, triggering the same inflammatory cascade that would fight an infection.
The inflammatory response involves a chain of proteins activating each other like dominoes. IRAK4 (interleukin-1 receptor-associated kinase 4) sits near the beginning of this chain, acting as a critical amplifier of the inflammatory signal. When IRAK4 is activated, it triggers downstream production of inflammatory cytokines including tumor necrosis factor-alpha (TNF-α) and interleukin-6 (IL-6). These cytokines interfere directly with insulin signaling in muscle, fat, and liver cells, reducing their ability to absorb glucose from the bloodstream in response to insulin.

In a healthy metabolic state, this inflammatory response is transient and resolves quickly. But when high-fat meals are frequent, the inflammation becomes chronic. Fat cells themselves begin secreting inflammatory cytokines, creating a self-perpetuating cycle. The immune cells residing in fat tissue shift from anti-inflammatory types (M2 macrophages) to pro-inflammatory types (M1 macrophages). This ongoing inflammation keeps insulin signaling impaired, forcing the pancreas to produce ever-higher amounts of insulin to achieve the same glucose-clearing effect. Eventually, even maximum insulin production isn’t enough, blood sugar rises, and Type 2 diabetes develops.
This understanding explains why diabetes rates have exploded alongside the Western diet’s shift toward processed foods high in both saturated fats and refined carbohydrates. It also explains why losing weight, particularly visceral fat around the organs, can reverse early diabetes: reducing fat tissue reduces the inflammatory burden. But it left researchers searching for ways to interrupt the inflammation directly, without requiring the weight loss that most people struggle to achieve and maintain.
The TMA Discovery: A Metabolite That Reprograms Inflammation
The research team’s investigation began with an observation that seemed counterintuitive. TMA had previously been studied primarily as a precursor to TMAO (trimethylamine N-oxide), a compound associated with increased cardiovascular risk. The assumption was that TMA was merely a metabolic intermediate with no significant biological activity of its own. But when the researchers screened compounds for their ability to block IRAK4, TMA emerged as a surprisingly potent inhibitor.
Using a combination of human cell models, mouse studies, and molecular target screening, the team demonstrated that TMA binds directly to IRAK4 and blocks its kinase activity. In cell cultures exposed to saturated fatty acids, TMA treatment prevented the inflammatory cytokine surge that would normally occur. In mice fed high-fat diets, enhancing TMA production through specific gut bacteria reduced inflammatory markers and improved insulin sensitivity, even without changes in body weight or fat mass.
The mechanism is elegantly specific. TMA doesn’t broadly suppress the immune system in ways that would leave you vulnerable to infections. Instead, it selectively blocks the inflammatory pathway activated by dietary fats while leaving other immune functions intact. This specificity makes it a particularly attractive target for therapeutic development. Unlike immunosuppressive drugs with wide-ranging side effects, a TMA-mimicking therapy could potentially block metabolic inflammation without compromising immune defense.
The discovery also reveals why the gut microbiome has such profound effects on metabolic health. Different bacterial species produce varying amounts of TMA from dietary precursors. Your microbiome composition determines how much TMA you generate from the same meal, which determines how strongly your immune system reacts to dietary fats, which determines your trajectory toward or away from insulin resistance. This explains some of the individual variation in diabetes risk that couldn’t be explained by diet and exercise alone.
Implications for Diabetes Prevention and Treatment
The immediate practical implication is that microbiome-targeted interventions could become a viable diabetes prevention strategy. Rather than asking people to maintain perfect diets indefinitely, something that most cannot do, healthcare providers might eventually be able to enhance the protective bacterial populations in patients’ guts. This could involve specific probiotic strains known to produce TMA, prebiotic fiber compounds that selectively feed TMA-producing bacteria, or even defined bacterial communities designed to optimize metabolic protection.
For people already diagnosed with Type 2 diabetes or prediabetes, this research suggests new pharmaceutical targets. Drug developers could create small molecules that mimic TMA’s binding to IRAK4, providing the same inflammatory protection without requiring changes to the gut microbiome. Given IRAK4’s well-characterized structure and the clear mechanism demonstrated in this study, such drug development is far more tractable than targeting vague concepts like “metabolic dysfunction.”

The research also reinforces the importance of existing gut health strategies for metabolic health. Our earlier coverage of gut health reset protocols and fermented foods gains additional mechanistic support from this discovery. While we don’t yet know exactly which bacterial strains are the most potent TMA producers, the general principle that diverse, fiber-fed microbiomes support metabolic health is now supported by an additional specific mechanism.
Importantly, this study helps explain why some people seem metabolically protected despite dietary patterns that cause problems for others. Individual microbiome composition creates significant variation in how the body responds to dietary fats. This isn’t just about genetic luck; it’s about cultivatable bacterial populations that can be influenced through diet, probiotics, and potentially medical interventions. The person who “eats whatever they want” without developing diabetes may have a microbiome that produces abundant TMA and other protective metabolites.
What This Means for Your Metabolic Health Today
While TMA-based therapies remain years from clinical application, the research offers several actionable insights for current metabolic health management. First, supporting gut bacteria diversity and abundance remains a sound strategy for metabolic protection. Dietary fiber from varied plant sources feeds the bacterial populations that produce protective metabolites, including but not limited to TMA. Aiming for 25-35 grams of fiber daily from diverse sources creates the substrate for a protective microbiome.
Foods rich in the precursors that bacteria convert to TMA include eggs, fish, and red meat, specifically choline and L-carnitine. This creates an apparent paradox: the same foods associated with increased TMAO (the potentially harmful downstream metabolite) are also sources of potentially protective TMA. The resolution may lie in the balance of bacterial species. A healthy, diverse microbiome may handle these compounds differently than a dysbiotic one, producing protective metabolites rather than harmful ones. This is another reason why the overall dietary pattern matters more than any single food.

Reducing the inflammatory trigger load also makes sense pending microbiome-targeted therapies. While your gut bacteria can potentially neutralize some of the inflammatory response to dietary fats, reducing the trigger frequency and intensity gives them less work to do. This doesn’t mean avoiding all fats, but rather moderating saturated fat intake while emphasizing monounsaturated fats (olive oil, avocados) and omega-3 fatty acids (fatty fish, walnuts) that have anti-inflammatory rather than pro-inflammatory effects.
Exercise continues to earn its place as the most reliable metabolic intervention. Regular physical activity reduces inflammation through multiple mechanisms independent of weight loss, improves insulin sensitivity directly, and also positively influences gut microbiome composition. The connection between fitness and metabolic health now includes another pathway: exercise-induced changes in gut bacteria may enhance production of protective metabolites like TMA.
The Bigger Picture: Inflammation as the Common Pathway
This TMA-IRAK4 research fits into a broader reconceptualization of metabolic disease. The old model viewed diabetes as fundamentally about sugar: too much sugar in the blood, treated by reducing sugar intake or enhancing sugar removal through medication. The emerging model views diabetes as fundamentally about inflammation: chronic immune activation that impairs cellular function across multiple organ systems, with elevated blood sugar being a downstream consequence rather than the root cause.
This inflammatory model explains observations the sugar-centric model couldn’t. It explains why diabetes clusters with other inflammatory conditions: cardiovascular disease, non-alcoholic fatty liver disease, certain cancers, even Alzheimer’s disease (increasingly called “Type 3 diabetes” by some researchers). It explains why anti-inflammatory interventions, from lifestyle measures to medications like metformin, can improve metabolic health even without changing blood sugar directly. And it explains why some people develop diabetes without excessive sugar intake while others consume significant sugar without developing it.
The gut-inflammation-diabetes connection is just one thread in a larger tapestry connecting the microbiome to whole-body health. The same general framework, gut bacteria producing metabolites that influence immune function and disease risk, applies to mental health through the gut-brain axis, to cardiovascular disease, to autoimmune conditions, and to aging itself. What we’re witnessing is the emergence of microbiome medicine as a genuine therapeutic field, moving from vague “gut health” pronouncements to specific mechanisms, specific targets, and specific interventions.
The Bottom Line
The discovery that the gut metabolite TMA can block IRAK4 and prevent diet-induced inflammation represents a genuine breakthrough in our understanding of how Type 2 diabetes develops. This research provides a clear molecular mechanism linking gut bacteria to metabolic health and opens multiple pathways for future prevention and treatment strategies. While clinical applications remain in development, the findings reinforce the importance of nurturing a healthy, diverse gut microbiome as a foundation for metabolic resilience.
Next Steps:
- Prioritize dietary fiber (25-35g daily) from diverse plant sources to support gut bacteria diversity
- Include fermented foods regularly (kimchi, yogurt, kefir, sauerkraut) to provide beneficial bacteria
- Moderate saturated fat intake while emphasizing anti-inflammatory fats (olive oil, omega-3s)
- Maintain regular exercise, which independently improves both inflammation and gut microbiome composition
- Consider comprehensive metabolic blood work (fasting glucose, HbA1c, fasting insulin, inflammatory markers) to establish your baseline
The gut-inflammation-diabetes connection reveals that metabolic health isn’t just about what you eat, but about how your unique bacterial ecosystem processes what you eat. Supporting that ecosystem through proven dietary and lifestyle measures positions you to benefit from emerging targeted therapies while reducing your risk today.
Sources: Nature Metabolism 2025 (TMA-IRAK4 discovery, Imperial College London/University of Louvain/Ottawa Heart Institute collaboration), Cell 2024 (gut microbiome and metabolic inflammation), Journal of Clinical Investigation (IRAK4 pathway in insulin resistance), Diabetes Care (inflammation-driven diabetes models), Gut Microbes journal (dietary precursors of TMA production).