
Maria, a 52-year-old accountant, lost 45 pounds in six months on semaglutide. Her doctor celebrated the scale victory. Her bloodwork improved across nearly every marker: fasting glucose dropped, A1C normalized, triglycerides plummeted. By standard medical measures, the medication was working exactly as intended. What the scale and blood tests didn’t reveal was that 18 of those 45 pounds came from muscle and other lean tissue rather than fat. When Maria’s personal trainer ran a body composition scan, the results told a different story: her body fat percentage had barely changed despite significant weight loss. She was lighter but proportionally fattier, weaker in the gym, and more fatigued than before starting the medication.
Maria’s experience represents a widespread but under-discussed phenomenon emerging from the GLP-1 medication revolution. Clinical trials of semaglutide (sold as Ozempic and Wegovy) and tirzepatide (Mounjaro and Zepbound) report that 25-40% of total weight lost comes from lean mass rather than fat. Traditional diet-induced weight loss typically runs 75% fat and 25% lean mass; the accelerated, appetite-suppressed weight loss these medications produce shifts that ratio unfavorably unless specific nutritional and exercise interventions are implemented.
The core problem is straightforward: when appetite suppression is so profound that people struggle to eat 800-1,200 calories daily, hitting adequate protein intake to preserve muscle becomes extremely challenging. The body, receiving insufficient protein and insufficient overall calories, draws on muscle tissue for amino acids and energy. Add the absence of resistance training stimulus, and muscle loss accelerates further. The scale drops, but the functional capacity, metabolic rate, and long-term health trajectory may suffer.
This article provides the evidence-based nutritional strategy for people using GLP-1 medications to ensure weight loss comes predominantly from fat rather than muscle, micronutrient deficiencies are prevented, and the metabolic improvements these medications can produce are maximized rather than undermined.
Understanding the Appetite Suppression Mechanism
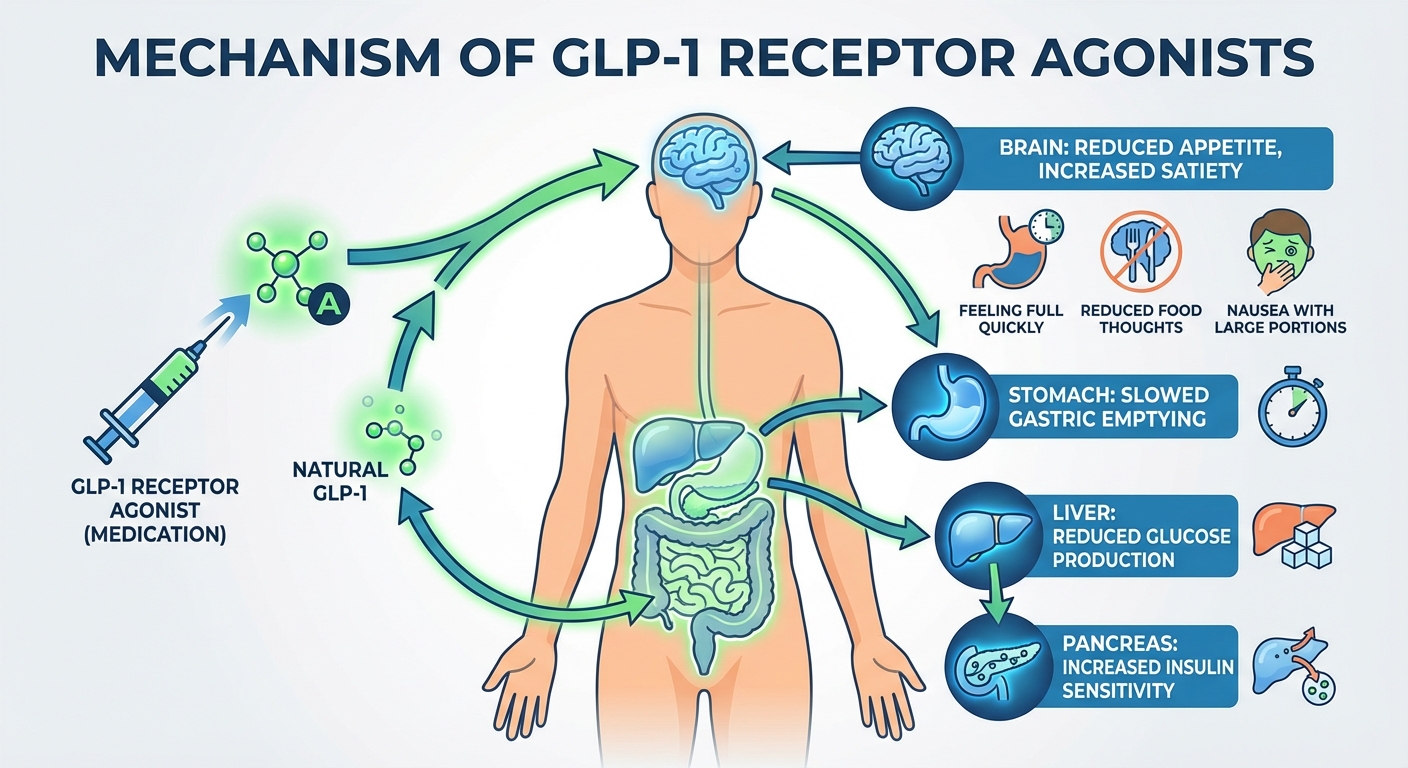
GLP-1 (glucagon-like peptide-1) is a hormone naturally produced in the intestines after eating. It signals satiety to the brain, slows gastric emptying so food remains in the stomach longer, enhances insulin secretion, and reduces glucagon (a hormone that raises blood sugar). These combined effects make you feel full, reduce hunger, and improve glucose regulation. The medications amplify these natural signals dramatically, creating appetite suppression far beyond what lifestyle interventions typically achieve.
People on GLP-1 medications commonly describe the experience as “food noise” disappearing. The constant background thoughts about what to eat, when to eat, cravings, and food preoccupation simply quiet. Many experience genuine disinterest in eating, where meals feel more like obligations than pleasures. Small portions produce extreme fullness. Larger portions trigger nausea. Food preferences often shift toward simpler, blander options as rich or complex foods become unappealing.
This profound appetite suppression produces the dramatic weight loss these medications are known for, averaging 15-20% of body weight over 12-18 months in clinical trials. But the same mechanism that enables this weight loss creates the nutritional challenge: when your body signals extreme fullness after 300-400 calories, eating the 1,200-1,500 calories and 100+ grams of protein needed to preserve muscle becomes genuinely difficult. Many people aren’t choosing to under-eat; they physiologically cannot eat more without severe discomfort.
Understanding this mechanism is essential for approaching nutrition strategically rather than intuitively. Normal hunger cues that would prompt adequate eating are suppressed. You cannot rely on appetite to guide intake. Instead, nutrition on GLP-1 medications requires deliberate planning, tracking, and sometimes eating despite absence of hunger or even in the presence of mild fullness.
The Muscle Preservation Imperative
The clinical data on body composition during GLP-1-mediated weight loss demands attention. A sub-study of the STEP 1 trial analyzing semaglutide found that lean mass comprised approximately 39% of total weight lost, substantially higher than the 20-25% typical of moderate caloric restriction. The SURMOUNT trials for tirzepatide showed similar patterns. These aren’t minor variations; losing 40% of weight as muscle versus 25% profoundly affects metabolic rate, functional capacity, and long-term outcomes.
Muscle tissue burns approximately 6 calories per pound per day at rest, while fat tissue burns only 2 calories. Losing 15 pounds of muscle versus 15 pounds of fat means your resting metabolic rate drops by an additional 60 calories daily. This may seem small, but over months and years, the accumulated metabolic deficit makes weight maintenance progressively harder. Add the functional implications: reduced strength for daily activities, higher injury risk, accelerated sarcopenia (age-related muscle wasting), and decreased bone density (muscle pulling on bone maintains bone mass), and the case for muscle preservation becomes compelling.
The encouraging news is that muscle loss on GLP-1 medications appears largely preventable with appropriate interventions. A 2024 study in Obesity found that GLP-1 users who performed resistance training twice weekly and consumed adequate protein (1.2+ grams per kilogram body weight) preserved 60-70% more lean mass than those who didn’t. The medication doesn’t force muscle loss; the nutritional and behavioral context determines body composition outcomes. People who eat adequate protein and strength train lose primarily fat. People who don’t lose substantial muscle alongside their fat.
The practical implication is clear: resistance training and protein intake aren’t optional enhancements for people on GLP-1 medications. They’re essential interventions that determine whether the medication produces healthy body composition changes or merely lower scale numbers with unchanged or worsened fat-to-muscle ratios.
Protein Targeting Strategy
Protein intake is the single highest-priority nutritional intervention for preserving muscle during GLP-1-mediated weight loss. The target range is 1.2-1.6 grams of protein per kilogram of goal body weight daily. Note this is goal weight, not current weight; someone currently weighing 200 pounds targeting 160 pounds (73 kg) should aim for 88-117 grams of protein daily.
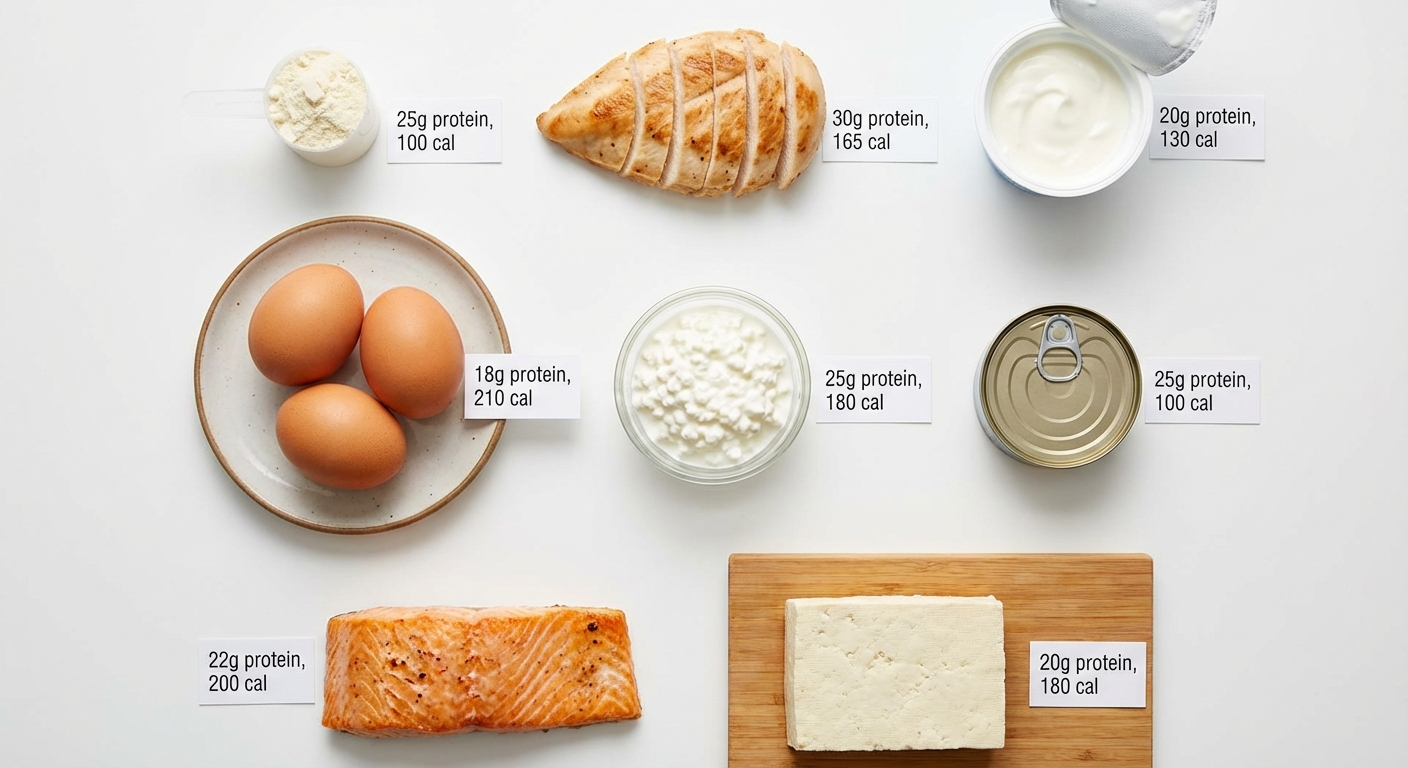
This target sounds manageable until you attempt to achieve it while eating 1,000-1,200 total calories and feeling full after every few bites. A chicken breast provides 30-35 grams of protein but also 150+ calories and significant volume in the stomach. Hitting 100 grams of protein means eating three chicken breast equivalents daily, consuming roughly half your caloric budget before vegetables, grains, or any other foods. For many people on GLP-1 medications, whole-food protein sources alone cannot practically deliver adequate protein within their caloric and volume tolerances.
This is where protein supplementation becomes genuinely necessary rather than merely convenient. Whey protein isolate provides 25-30 grams of protein in 100-120 calories, a dramatically better protein-to-calorie and protein-to-volume ratio than whole foods. A protein shake in the morning, consuming minimal stomach space and requiring no chewing, can deliver one-third of daily protein needs in minutes. Casein protein before bed provides slow-digesting protein that supports muscle synthesis overnight. For people who cannot tolerate dairy, plant-based protein powders (pea, rice, or blends) offer alternatives.
The practical strategy involves protein at every eating occasion, prioritized before other macronutrients. Eat protein first when you sit down to meals, while you still have appetite and stomach capacity. Choose protein-dense foods: Greek yogurt (20 grams per cup), cottage cheese (25 grams per cup), eggs (6 grams each), chicken (30 grams per 4 oz), fish (25-30 grams per 4 oz). Use shakes to fill gaps when solid food intake falls short. Track protein intake at least initially to ensure targets are met; estimation without tracking typically underestimates actual consumption significantly.
Our comprehensive guide on protein requirements for different goals covers the science of protein needs in depth, while our protein timing article addresses optimal distribution throughout the day.
Micronutrient Deficiency Prevention
Severely restricted caloric intake creates real risk of micronutrient deficiencies. When eating 1,000-1,200 calories daily, even with excellent food choices, meeting all vitamin and mineral needs through food alone becomes mathematically challenging. The body requires similar micronutrient quantities regardless of caloric intake; cutting calories in half doesn’t cut micronutrient needs in half.
Iron deficiency deserves particular attention, especially for menstruating women. Iron absorption requires adequate stomach acid and is impaired by many foods and supplements. With reduced meat intake (common due to texture and volume issues on GLP-1s) and overall lower food volume, iron status often declines. Symptoms include fatigue, weakness, pale skin, and difficulty concentrating. Ferritin levels should be checked every 3-6 months, with supplementation if levels drop below 50-70 ng/mL.
Vitamin B12 deficiency emerges when animal product intake drops. Since B12 is found exclusively in animal foods (or fortified products), reduced consumption of meat, dairy, and eggs directly reduces B12 intake. Symptoms of deficiency include fatigue, neurological issues, and cognitive problems that may be attributed to the medication itself rather than nutritional status. Supplementation with methylcobalamin (the active B12 form) is reasonable for most people eating less than 1,500 calories daily.
Vitamin D, calcium, and magnesium status all warrant attention. Reduced dairy consumption (common due to volume and texture issues) decreases calcium and vitamin D intake. Magnesium, found in leafy greens, nuts, and whole grains, is easily under-consumed when total food volume is low. These minerals support bone health, muscle function, and metabolic regulation.
A practical prevention strategy includes a high-quality multivitamin providing 100% of daily values for most micronutrients, additional vitamin D3 (2,000-5,000 IU daily, adjusted based on blood levels), and magnesium supplementation (200-400 mg daily, preferably glycinate or citrate forms). Blood work every 3-6 months checking vitamin D, B12, iron/ferritin, and basic metabolic panels identifies developing deficiencies before symptoms emerge.
Strength Training as Non-Negotiable Intervention
Adequate protein provides the raw materials for muscle preservation; resistance training provides the signal that tells the body to maintain muscle rather than catabolize it for energy. Without the mechanical stimulus of strength training, the body has no reason to prioritize muscle tissue during caloric deficit. With consistent resistance training, the body receives the message that muscle is needed and should be preserved.
The evidence is compelling. Studies of GLP-1 users comparing those who strength train to those who don’t show that trained individuals retain 60-70% more lean mass during equivalent weight loss. This isn’t a subtle effect; it’s the difference between losing primarily fat versus losing substantial amounts of both fat and muscle. Resistance training transforms the body composition outcomes of these medications.
The minimum effective dose is two full-body strength training sessions weekly, focusing on compound movements that engage multiple muscle groups: squats, deadlifts, lunges, presses, rows, and pull-downs. Each session should include 2-3 sets of 6-12 repetitions for major movement patterns, with weight heavy enough that the final repetitions of each set are challenging. Sessions of 30-45 minutes are sufficient; elaborate programs aren’t necessary. What matters is consistency and progressive overload (gradually increasing weight or repetitions over time).
People new to strength training should consider working with a qualified trainer initially to learn proper form and develop a sustainable program. Those with physical limitations or injuries should work with their healthcare provider to identify appropriate exercises. The specific exercises matter less than the presence of resistance training stimulus; any program that challenges muscles twice weekly dramatically improves outcomes compared to no resistance training.
For detailed programming guidance, our guide on strength training for adults over 50 provides age-appropriate protocols, while the article on strength training and aging covers the science of muscle preservation across the lifespan.

Managing Common Side Effects Through Nutrition
GLP-1 medications produce predictable side effects that nutritional strategies can often mitigate. Nausea, the most common complaint, particularly during dose escalation, responds to several interventions. Eating smaller portions more frequently rather than larger meals reduces the volume of food in the stomach at any time. Bland, simple foods (crackers, rice, bananas, toast) are often better tolerated than rich or complex dishes. Avoiding lying down immediately after eating allows gravity to assist gastric emptying. Ginger, whether as tea, supplements, or candied ginger, has evidence for nausea reduction. If nausea is severe, eating whatever you can tolerate to meet protein needs takes priority over food quality.
Constipation affects many people as food volume decreases and transit slows. Fiber intake, often reduced when overall food intake drops, should be maintained or increased through vegetables, fruits, and supplementation if needed. Adequate hydration (at least 8 cups daily, preferably 10+) is essential for digestive function. Magnesium supplementation (200-400 mg of citrate or glycinate) promotes healthy bowel function. Physical activity, even moderate walking, supports digestive motility. If constipation persists despite these measures, over-the-counter remedies like polyethylene glycol (MiraLAX) are generally safe for occasional use.
Extreme fullness after small portions is the defining challenge. The solution isn’t forcing larger portions, which causes discomfort and may trigger vomiting, but rather optimizing what you eat within your capacity. Choose calorie-dense, protein-rich foods over high-volume, low-calorie options when meeting nutritional targets is challenging. Drink fluids between meals rather than with meals (liquids occupy stomach space that could hold food). Accept that eating may feel like a chore rather than a pleasure, and eat by plan rather than by appetite.
Sample Meal Structure
A practical daily eating pattern for someone on GLP-1 medication targeting 1,200 calories and 100 grams of protein might look like this structure. The specific foods should be adjusted based on individual tolerances and preferences, but the framework illustrates how to hit nutritional targets within severe caloric constraints.
Breakfast provides 300 calories and 30 grams of protein. Options include a protein shake made with whey isolate, milk or water, and a small banana; or Greek yogurt with berries and a small handful of granola; or three eggs prepared however tolerated. The priority is protein first thing in the morning to begin the day on track.
Mid-morning, if any capacity exists, provides another 15-20 grams of protein through 150-200 calories. Cottage cheese with fruit, a small protein bar, or a handful of nuts and cheese work here. If appetite is absent, skip and redistribute protein to other meals.
Lunch provides 350 calories and 35 grams of protein. A palm-sized portion of grilled chicken (4 oz) with a large vegetable salad and light dressing; or tuna over greens with olive oil; or a turkey and cheese wrap on a low-carb tortilla. Vegetables add volume and nutrients without excessive calories.
Afternoon snack, if tolerated, provides 100-150 calories and 15 grams of protein. Hard-boiled eggs, deli meat roll-ups with cheese, or a small protein shake address this. Again, skip if capacity is absent and redistribute.
Dinner provides 350-400 calories and 30 grams of protein. Salmon or other fish (4-5 oz) with roasted vegetables; lean beef stir-fry with minimal rice and lots of vegetables; or tofu with vegetables and a small portion of whole grains. Eating dinner earlier (before 7 PM if possible) allows digestion before bed and may reduce nighttime discomfort.
Pre-bed, if muscle preservation is priority and evening eating is tolerated, casein protein (20-25 grams) provides slow-release amino acids overnight. This is optional but beneficial.
Long-Term Sustainability Considerations
GLP-1 medications are increasingly recognized as long-term or lifelong treatments for many people. Studies show that stopping the medication typically results in weight regain as appetite returns to baseline. This means the nutritional strategies aren’t temporary adjustments but permanent lifestyle modifications.
Caloric intake should gradually increase as tolerated, aiming for at least 1,200-1,500 calories daily once past initial adjustment phases. Sustained intake below 1,000 calories produces nutrient deficiencies, fatigue, and metabolic adaptation that impair long-term health regardless of weight status. If you cannot eat 1,200 calories without severe discomfort after several months, discuss dose adjustment with your prescriber.
Food variety prevents both nutrient gaps and psychological burnout. The tendency to default to a small rotation of “safe” tolerated foods is understandable but creates monotony that undermines adherence over years. Experiment regularly with new foods and preparations. Some foods that were aversive initially may become tolerable over time as the body adapts to the medication.
Social eating requires adaptation rather than avoidance. Strategies include eating a small protein-focused portion slowly, choosing protein-forward menu items, and accepting that you won’t eat the same volume as companions. Complete avoidance of social eating is neither necessary nor healthy for long-term wellbeing.
Regular monitoring through blood work (every 3-6 months) and body composition assessment (DEXA scan annually) provides objective feedback on nutritional status and body composition trajectories. These measures identify problems before they become severe and allow intervention adjustments.
The Bottom Line
GLP-1 medications produce remarkable weight loss, but the quality of that weight loss depends entirely on nutritional and exercise context. Without intervention, 25-40% of weight lost is muscle, undermining metabolic rate, functional capacity, and long-term outcomes. With proper protein intake and resistance training, weight loss shifts toward 75-80% fat, producing genuinely healthier body composition.
The essential interventions are non-negotiable: protein intake of 1.2-1.6 grams per kilogram of goal body weight daily, resistance training at least twice weekly, comprehensive micronutrient supplementation, and adequate total caloric intake (minimum 1,200 calories for most people). These aren’t optional enhancements; they determine whether the medication produces healthy weight loss or merely lower numbers on a scale with unchanged or worsened metabolic health.
Your GLP-1 Nutrition Protocol:
- Calculate protein target: multiply goal weight in kg by 1.2-1.6 for daily grams
- Track protein intake for at least the first month to ensure targets are met
- Use protein supplements (shakes, bars) when whole food intake is insufficient
- Begin or continue resistance training: 2-3 sessions weekly, compound movements
- Take a comprehensive multivitamin plus vitamin D (2,000-5,000 IU) and magnesium (200-400 mg)
- Monitor blood work every 3-6 months for developing deficiencies
- Aim for minimum 1,200 calories daily; discuss with prescriber if this is impossible
- Get annual DEXA scan to track body composition, not just scale weight
Sources: STEP clinical trials body composition data, SURMOUNT tirzepatide studies, Obesity journal research on resistance training and GLP-1 outcomes, protein requirements meta-analyses for rapid weight loss, American Society for Metabolic and Bariatric Surgery nutrition guidelines adapted for GLP-1 use.





